Dr Josep Iglesies-Grau, M.D., Ph.D.
Centre de recherche et Centre ÉPIC, Institut de cardiologie de Montréal. Département de Médecine, Université de Montréal, Montréal, Québec, Canada, Département de Nutrition, Université de Montréal, Montréal, Québec, Canada
See all articlesOverview
- It is difficult to lose weight, and especially to maintain these losses over the long term, due to a series of adaptations the body makes as it works hard to combat the depletion of this energy reserve and maintain the initial weight.
- This phenomenon is also observed with the newer GLP-1 agonists (Ozempic, Mounjaro), with significant weight regain occurring after treatment is stopped.
- The prevention of the many diseases that result from being overweight cannot therefore rely solely on taking medication; a healthy diet, mainly composed of plants and free from high-calorie processed foods, remains absolutely essential for obesity management.
It is now undeniable that excessive fat accumulation is a major risk factor for chronic diseases affecting a significant proportion of the population, including cardiovascular disease, type 2 diabetes, dementia, and several types of cancer. For people suffering from obesity, weight loss therefore represents a very promising avenue for reducing the incidence and progression of many of these conditions. This is particularly true with regard to cardiovascular disease, where a weight loss as small as 5% of the initial weight can reverse many of the harmful cardiometabolic effects associated with excess adiposity.
Recent studies clearly show that the only real way to achieve significant weight loss, and especially to maintain these losses long-term, relies largely on a sustained reduction in energy intake. However, this goal is difficult for most people to achieve, particularly in environments where food is plentiful and readily available. Consequently, even if these diets generally lead to short-term weight loss, this loss is very often temporary, and partial or complete weight regain can occur over time, regardless of the nutritional approaches used.
The memory of obesity
Contrary to some still widespread perceptions, this weight regain has absolutely nothing to do with a supposed lack of willpower on the part of people living with excess weight. Research over the last few decades has clearly shown that fat loss triggers a series of highly complex metabolic, hormonal, and neurological adaptations designed to combat the depletion of this energy reserve and maintain the initial weight. In other words, the body possesses a form of “obesity memory” that makes maintaining weight loss in the long term extremely difficult, regardless of the method used to reduce body weight. At least four major factors contribute to this memory (Figure 1):
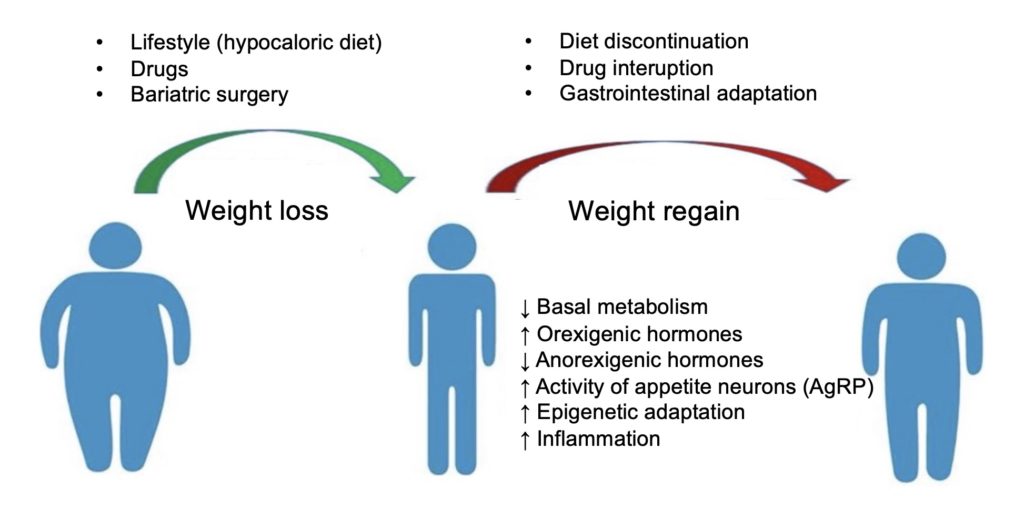
- Reduction of basal metabolic rate. 60 to 75% of our total energy expenditure comes from basal metabolism, that is, the amount of energy expended to maintain vital functions at rest. After weight loss, this basal energy expenditure can decrease dramatically (by up to 700 kcal per day), so that even a normal calorie intake can exceed the body’s needs and contribute to weight gain. This phenomenon is an adaptation that developed over the course of evolution to survive famine: in response to a drastic decrease in available calories (as in the case of a severe low-calorie diet), basal metabolism becomes much more efficient and produces more energy (in the form of ATP) with less heat loss, thus preserving energy reserves in the long term.
- Increased appetite. The response to significant weight loss, which the brain interprets as starvation, is also characterized by profound and persistent changes in the hormones involved in appetite regulation. For example, there is an increase in appetite-stimulating (orexigenic) hormones such as ghrelin and a parallel reduction in appetite-suppressing (anorexigenic) hormones such as PYY, cholecystokinin (CCK), amylin, and leptin. These compensatory variations lead to an increase in appetite that is difficult to control, characterized by cravings, hypersensitivity to the smell or even the sight of food, and excessive pleasure derived from its consumption (hedonic value). Weight loss also appears to cause strong stimulation of orexigenic neurons (AgRPs) in the hypothalamus, thus triggering a sustained increase in food intake and a regaining of the lost weight.
- Genetic memory of obesity. Repeated exposure to excess calories causes fat cells (adipocytes) to enlarge in order to store this surplus energy. Adipocytes are extremely flexible cells and can modify the expression of several genes to allow this growth. These changes are retained in memory (epigenetic adaptation), so that after the end of a weight-loss treatment, the adipocytes are already “programmed” to store excess energy if the number of calories exceeds the body’s needs.
- Inflammation at the adipocyte level. The expansion of adipose tissue can be interpreted as an attack by the immune system, leading to the infiltration of several pro-inflammatory cells and the creation of a climate of chronic inflammation that affects adipocyte function and promotes abnormal adipose tissue growth beyond the limits normally imposed by the tissue envelope (the extracellular matrix). These inflammatory cells remain present in adipose tissue even after significant weight loss, so subsequent exposure to excess calories caused by the metabolic and hormonal factors mentioned above will cause even more rapid fat accumulation than in adipocytes that have never been exposed to obesity, thus leading to post-weight regain (Figure 2). Recent studies suggest that this dysregulation of inflammation in response to obesity could last for several years due to a lasting adaptation of adaptive immune cells (CD4+ T lymphocytes) to the excessive accumulation of fat in adipose tissue.
For all these reasons, lasting reduction in body weight is generally a very difficult goal to achieve for many people, especially when the level of adiposity is high.
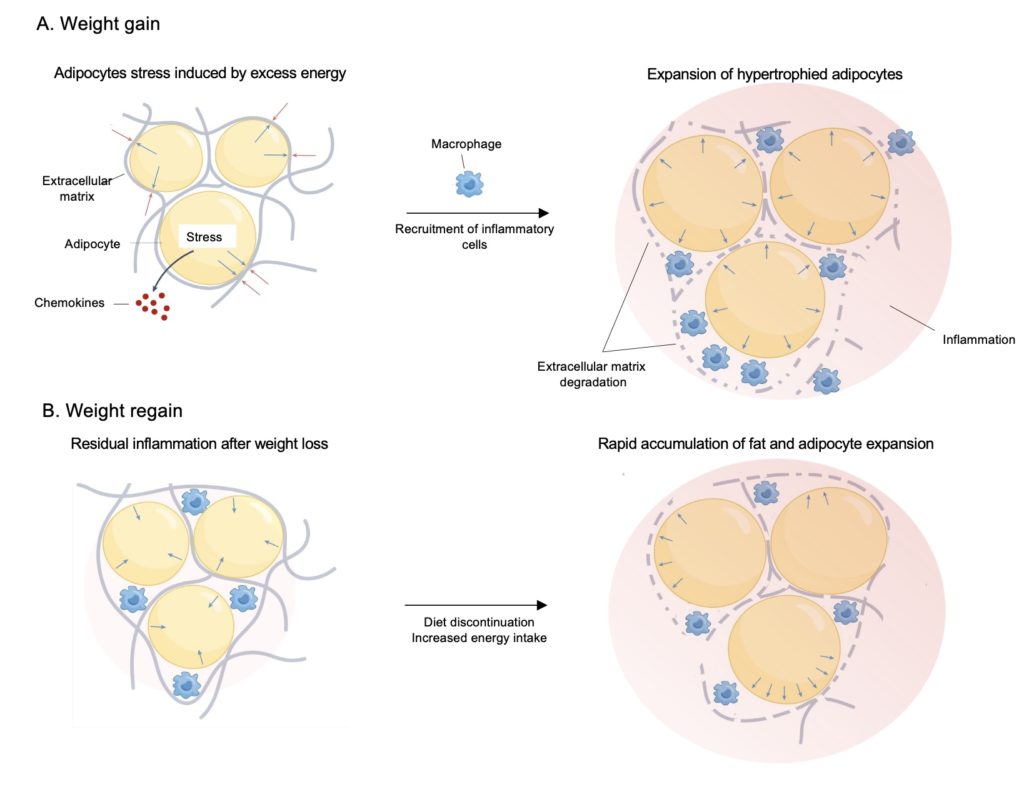
A. A positive energy balance leads to the expansion of adipocytes, which generates stress at the points of contact with the extracellular matrix surrounding the adipose tissue and prevents its expansion (blue and red arrows). Chemokines are then secreted by the adipocytes to attract inflammatory cells (macrophages), and this recruitment causes local inflammation (illustrated in red) and the secretion of enzymes that degrade the matrix, weakening it and allowing further adipocyte expansion.
B. After weight loss, the size of adipocytes decreases, and the regenerated matrix tightens around the atrophied adipocytes. However, some macrophages remain in the adipose tissue and, in the event of renewed overeating, are already present to secrete matrix-degrading enzymes, which promotes rapid adipocyte proliferation and weight regain. Adapted from van Baak and Mariman (2023).
Yo-yo effect
In addition to being extremely discouraging, these weight regains also seem to have negative health effects, especially when they occur repeatedly. These repeated weight fluctuations, known as the “yo-yo effect” (an analogy to the toy that goes up and down), can affect up to 50% of the adult population, and several studies (but not all, see here for example) have reported an increased risk of various diseases in people whose weight fluctuates the most. For example, recent meta-analyses have shown that weight fluctuations increase the risk of high blood pressure (hypertension), cardiovascular disease, type 2 diabetes (T2D), and all-cause mortality. The mechanisms involved remain to be identified, but it has been proposed in the case of cardiovascular disease that repeated cycles of weight loss and gain lead to abnormal fluctuations in several risk factors such as blood pressure, heart rate, cardiac workload, sympathetic activity, blood glucose, and lipid profile. The stress induced by repeated variations in these variables would impose an additional load on the heart and could therefore lead to vascular damage resulting in the development of atherosclerosis.
GLP-1 agonists
The recent popularity of GLP-1 agonists (Ozempic, Wegovy, Mounjaro, Zepbound) has brought to light the problem of weight regain after treatment-induced weight loss. As described in more detail, these medications are analogs of a hormone secreted by the intestine (GLP-1) that were initially developed to improve blood glucose control in patients with type 2 diabetes.
These medications are now primarily known for their significant effects on weight loss, with reductions in body weight reaching 15–20% in some cases, much greater than the losses achieved through lifestyle modifications (diet, exercise) or with the first generation of medications used for weight management (Figure 3). The effectiveness of GLP-1 medications for weight loss appears to be primarily due to their direct action on the processes involved in controlling eating behaviour. This includes a significant decrease in appetite, a reduction in caloric intake of approximately 30%, and a slowing of gastric emptying, which promotes an earlier and more prolonged feeling of fullness, sometimes accompanied by nausea, even after small meals. Therefore, the substantial energy deficit resulting from the mechanism of action of these medications is thought to be directly responsible for the significant weight loss observed in studies, confirming that a significant reduction in caloric intake largely determines weight loss.
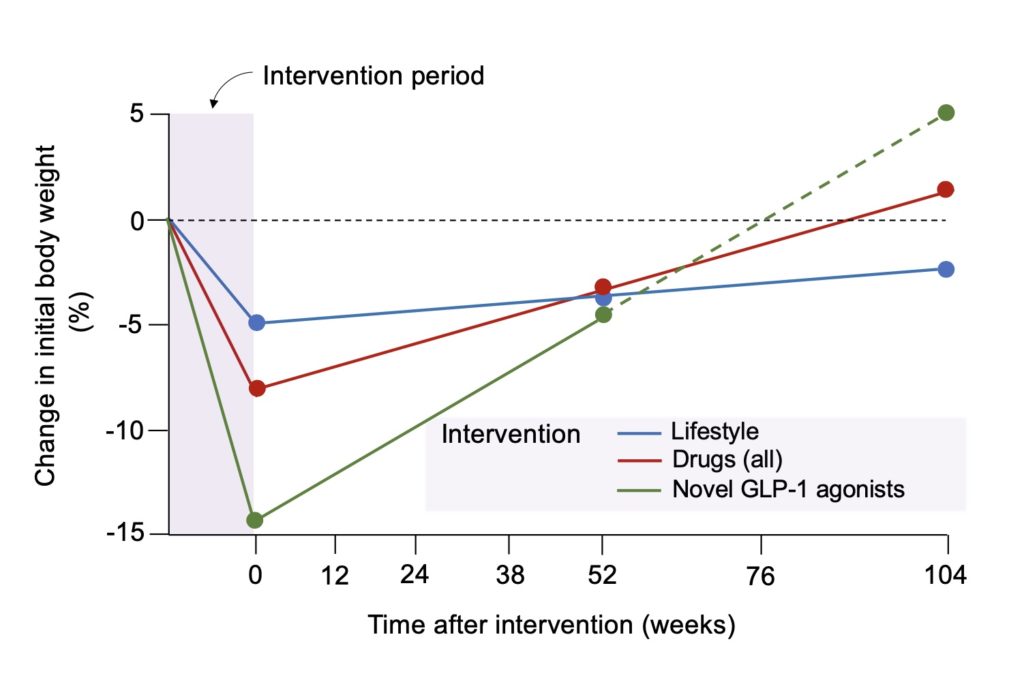
Despite their short-term efficacy, GLP-1 agonists present the same problem that affects all long-term weight-loss treatments: discontinuation of treatment is generally followed by considerable weight regain, with approximately two-thirds of the lost weight regained within the following year (Figure 3). Consequently, the improvement in several health parameters resulting from weight loss can be reversed by a significant deterioration in several parameters associated with being overweight, including blood pressure and adequate blood glucose control.
This situation raises certain clinical challenges, as it is difficult to imagine administering these medications over very long periods to prevent relapses. On the one hand, adherence to these medications remains quite low, with less than 50% of people continuing treatment beyond one year, mainly due to significant side effects (particularly gastrointestinal, such as nausea). On the other hand, the major loss of appetite in treated individuals considerably increases the risk of malnutrition, with a significant proportion of patients not meeting the minimum recommended intake levels for several essential nutrients. An increased risk of certain eating disorders (such as anorexia) has also been observed in individuals with a history of mental health or eating disorders, and therefore, close clinical monitoring is recommended to prevent a possible exacerbation of problematic eating behaviours.
In short, despite the current enthusiasm surrounding GLP-1 agonists, these medications cannot be presented as a miracle cure for a problem as complex as obesity. While significant weight loss, even temporary, may offer some health benefits to obese individuals, those using these agonists should be informed of their limitations, including the high rate of treatment discontinuation and the risk of weight regain after stopping treatment.
Combining treatments, diet, and a supportive environment
The dramatic increase in the number of overweight people observed in recent decades clearly demonstrates that the current obesity epidemic is closely linked to changes in our lifestyles, with the omnipresence of ultra-processed foods, the gradual loss of traditional eating and cooking habits, and the increase in sedentary behaviour and physical inactivity playing a significant role. A return to basics, based on a healthy diet primarily composed of plant-based foods and free from high-calorie processed foods, therefore remains absolutely essential for managing obesity. While not replacing these prerequisites, GLP-1 medications can nevertheless play a complementary role by enabling some individuals to achieve significant weight loss, which may have previously been difficult to attain. Adopting a healthier diet during treatment, combined with the numerous physical and psychological benefits of weight loss, could then serve as a springboard for maintaining this new lifestyle and preventing the weight regain associated with stopping treatment.
Finally, society also has an important role to play in changing the obesogenic environment in which we live. Effective public health measures, such as taxes on sugary drinks, clear food labelling, and policies facilitating access to fruits, vegetables, and fresh foods, should be implemented to sustainably support improvements in diet quality and make healthy choices simpler, more accessible, and more sustainable. Preventing obesity cannot rely solely on individuals or depend solely on medication; it also requires building an environment that makes health possible.