Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesOverview
- Semaglutide and tirzepatide are peptides similar to two hormones produced by the digestive system, namely glucagon-like peptide-1 (GLP-1) and glucose‐dependent insulinotropic polypeptide (GIP).
- In addition to improving glycemic control, the administration of these drugs causes a drastic drop in appetite and caloric intake.
- These effects result in very significant weight loss (15-20% of initial body weight), i.e., of the same order of magnitude as that obtained by bariatric surgery.
The prevalence of overweight has increased dramatically in recent decades, with nearly 2 billion people who are overweight, including 650 million obese. This is an unprecedented global health crisis, which imposes a considerable burden on health systems. Excess weight promotes the development of a wide range of pathologies (insulin resistance, hypertension, chronic inflammation, dyslipidemia), which increase the risk of complications such as type 2 diabetes, cardiovascular disease, hepatic steatosis, several types of cancer and reduce life expectancy.
Overweight and obesity are fundamentally consequences of excessive caloric intake, but the ever-increasing number of overweight people, despite its well-documented negative health effects, shows that restoring this imbalance is not easy, especially in our time of food abundance. Although lifestyle interventions (low-calorie diets and exercise) are still the cornerstone of weight management, weight loss achieved through this approach is extremely difficult to sustain in the long term, particularly due to physiological adaptations that reduce the energy expended or increase appetite to compensate for the missing calories. In other words, once obesity has set in for a long time, these mechanisms make it very difficult to return to a lower weight.
To overcome these limitations, a number of pharmacological approaches have been developed over the past decades, but these drugs are generally of fairly limited efficacy, expensive and can in some cases cause significant side effects. Much more drastic approaches, bariatric surgery in particular, manage to generate significant and lasting weight loss, but these invasive procedures are inherently more risky and are generally restricted to people with morbid obesity (BMI> 40).
It is therefore in this context, where treatment options for obesity remain very limited, that the appearance of Ozempic® and Mounjaro™ on the market is currently generating enormous interest, both in the medical and scientific communities and in the general population. Although these two drugs were originally developed to improve glycemic control in people with type 2 diabetes, they simultaneously cause significant weight loss in these patients, without too many major side effects, and could therefore represent a new therapeutic strategy for the normalization of body weight.
A new pharmacological approach: The incretin effect
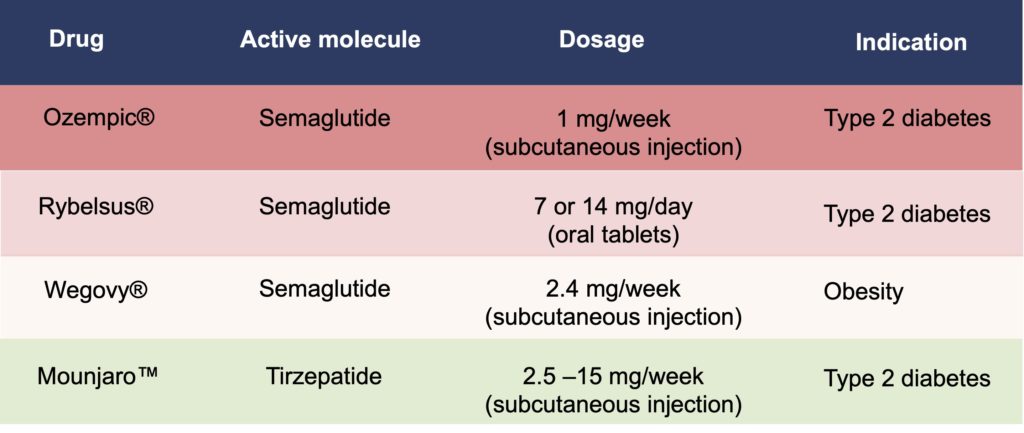
First of all, it should be noted that although they are best known to the public by their trade names (Ozempic®, Mounjaro™), it is the generic names of these drugs (semaglutide and tirzepatide, respectively) that are used in the scientific literature and we will therefore use this nomenclature throughout this article. The use of generic names also has the advantage of avoiding the confusion that can be generated by the different trade names given to drugs according to their mode of administration and/or therapeutic indication (Table 1).
Table 1. New antidiabetic and anti-obesity drugs. Note that the therapeutic indication for all of these drugs is for type 2 diabetes, with the exception of Wegovy® (2.4 mg/week of semaglutide by subcutaneous injection), which was recently approved for weight loss.
Semaglutide and tirzepatide are peptides (hence their names ending in “-ide”) analogous to two hormones produced by the digestive system, glucagon-like peptide-1 (GLP-1) and glucose‐dependent insulinotropic polypeptide (GIP). These peptides were designed to mimic the action of these hormones (what in pharmacology is called an agonist effect) on the control of glycemia. Following the absorption of sugar, GLP-1 and GIP secreted by cells of the intestine make it possible to very significantly increase the production of insulin by the pancreas, at levels much higher than those that are produced simply in response to the presence of sugar in the blood (Figure 1).
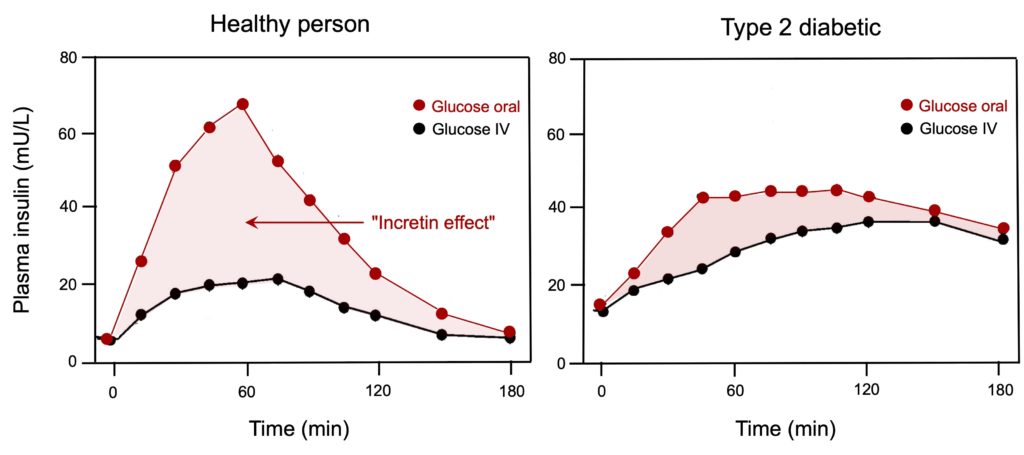
Figure 1. Variation in insulin response following bolus administration of glucose in metabolically healthy individuals or patients with type 2 diabetes. Values represent plasma insulin levels induced by glucose given orally (50 g/400 mL) (red circles) or an equivalent amount (isoglycemic) given intravenously (IV) (black circles). Note the large increase in insulin response caused by oral glucose compared to intravenous glucose in healthy people (light red area). This phenomenon, known as the “incretin effect,” is greatly reduced in diabetics, a difference that led to the development of analogues of incretin GLP-1 and GIP. Adapted from Nauck et al. (1986).
Historically, this increased insulin response mediated by GLP-1 and GIP had been attributed to factors termed “incretins” (derived from “incretion”, a term used at that time to refer to a secretion that remains inside the body), hence the name “incretin effect” is still used today to describe the rise in insulin mediated by the action of these hormones. It is an essential part of the insulin response to what we eat: in healthy people, it is estimated that around 70% of the insulin produced by the pancreas is a consequence of the incretin effect.
It is in this context that semaglutide and tirzepatide were developed. This incretin effect is considerably attenuated in people with type 2 diabetes (see Figure 1), a loss that is even considered an early indicator of the disease, but it was observed that this deficit could be completely corrected by the continuous infusion of GLP-1 to diabetic patients. It has therefore been postulated that the administration of molecules capable of mimicking the action of GLP-1 and/or GIP could reproduce this incretin effect and thus stimulate insulin production and improve glycemic control in type 2 diabetics. These efforts have led to the development of various GLP-1 receptor agonists, the most recent being semaglutide and tirzepatide, approved for the treatment of type 2 diabetes in 2018 and 2022, respectively.
Single and dual agonists
The fundamental difference between these two molecules is that semaglutide is a GLP-1 agonist, i.e., it has a strong structural similarity (95%) with this hormone and specifically activates its receptor, while tirzepatide is a dual agonist, i.e., it has a hybrid structure that allows it to activate both GLP-1 and GIP receptors (Figure 2). In both cases, modifications made to the structures of the peptides cause their bioavailability to be increased dramatically compared to the hormones secreted naturally by the intestine, from just a few minutes to more than a hundred hours, which allows these drugs to be administered by subcutaneous injection only once a week. It should also be noted that an oral form of semaglutide was developed by adding an agent to the drug formulation, which increases intestinal permeability, sodium N-(8-(2-hydroxybenzoyl)amino)caprylate (SNAC), but the lower bioavailability of the molecule requires daily administration to achieve glycemic control equivalent to that obtained by the form administered subcutaneously.
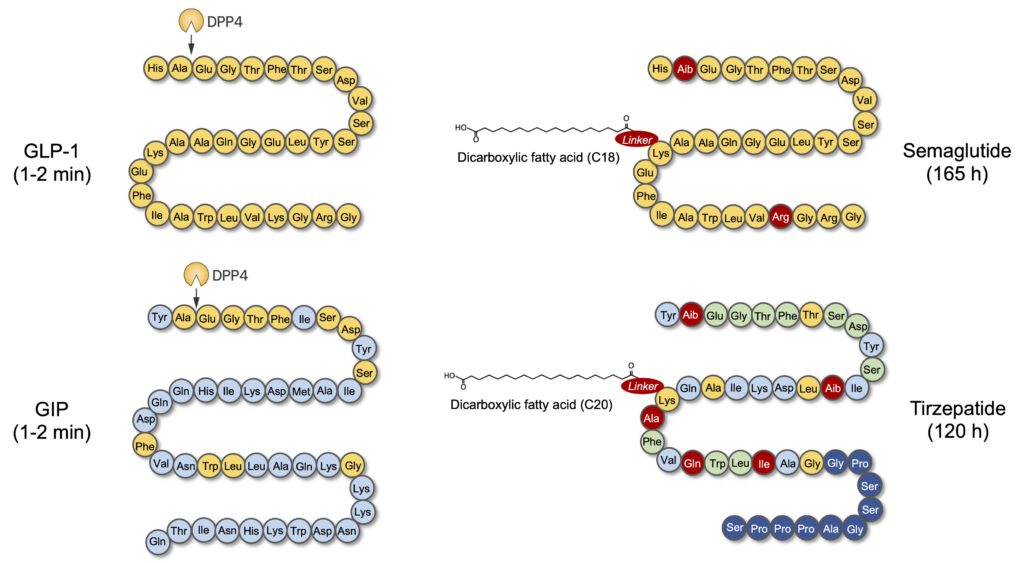
Figure 2. Structures of semaglutide and tirzepatide and their similarity to GLP-1 and GIP. GLP-1 is a 31 amino acid hormone (yellow circles), some of which are conserved in GIP, a 42 amino acid hormone (blue circles). Both hormones have a very short half-life (the time corresponding to a loss of half of their physiological activity), of only 1-2 minutes, in particular due to their degradation by dipeptidyl peptidase-4 (DPP-4). Two main strategies have been used to modify the sequences of semaglutide and tirzepatide (red circles) and increase their bioavailability: 1) removal of the DPP-4 cleavage site, replacing alanine with an analogous molecule (α-aminoisobutyric acid (Aib)), but not recognized by the enzyme; 2) the addition of a fatty acid using a “linker” to promote the binding of molecules to serum albumin and thus reduce their elimination at the renal level. Note that semaglutide is very similar to GLP-1 and its mechanism of action is therefore limited to the activation of the receptor for this hormone, while tirzepatide is made up of an amalgam of amino acids found both in the GLP-1 (yellow circles), GIP (blue circles), and in the two hormones (green circles), which gives it a double agonist activity, capable of activating both receptors for these hormones. The dark blue circles in the terminal portion of tirzepatide are amino acids from exenatide, a protein-derived peptide (exendin-4) present in the venom of the Gila monster (Heloderma suspectum) and known to activate the receptor GLP-1.
These structural differences between semaglutide and tirzepatide obviously have consequences for their biological actions. Since semaglutide is a “pure” agonist of the GLP-1 receptor, it exclusively stimulates the phenomena controlled by this receptor, while the ability of tirzepatide to act simultaneously on the GLP-1 and GIP receptors enables the activation of all the processes mediated by these incretins (Figure 3).
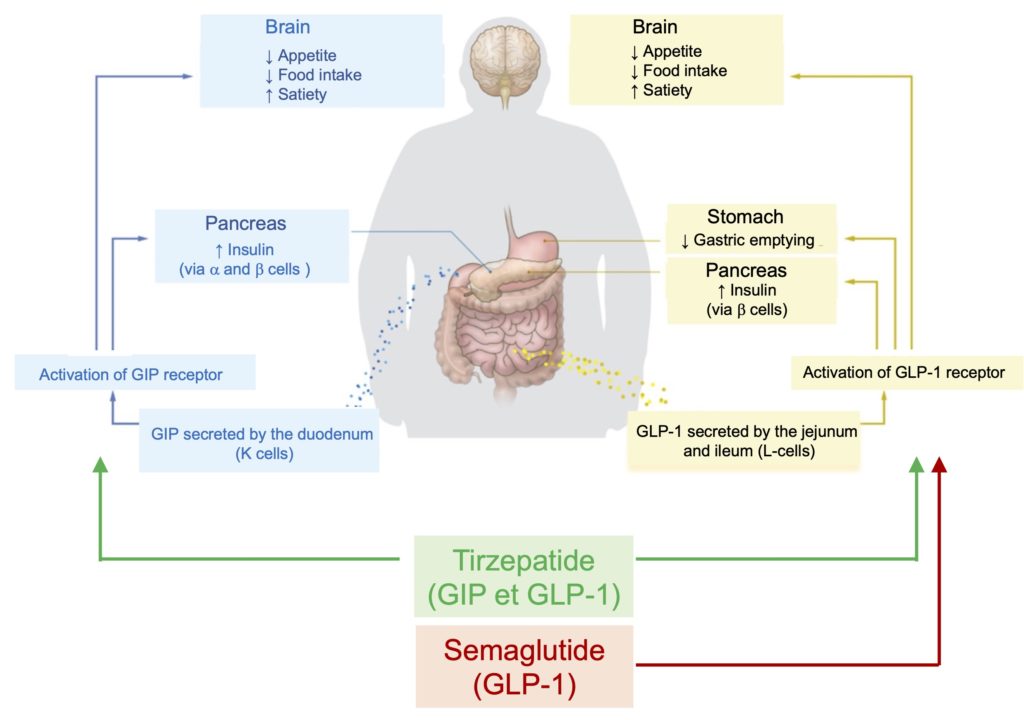
Figure 3. Mechanisms of action of GIP, GLP-1 and their agonists. Adapted from Bass et al. (2023).
As mentioned earlier, the most important effect of incretins is to stimulate the production and secretion of insulin by the pancreas, and clinical studies show that the activation of this process, whether by stimulation of GLP-1 by semaglutide alone or simultaneous stimulation of GLP-1/GIP by tirzepatide, is associated with better glycemic control in type 2 diabetics. In this respect, the dual agonist effect of tirzepatide seems to give it a superiority on semaglutide, with a greater decrease (more than 2%) in glycated hemoglobin (A1c), a marker of chronic hyperglycemia (Figure 4). For comparison, the improvement in glycemic control following bariatric surgery is of the same order, with a decrease in A1c varying between 1.8 and 3.5%.
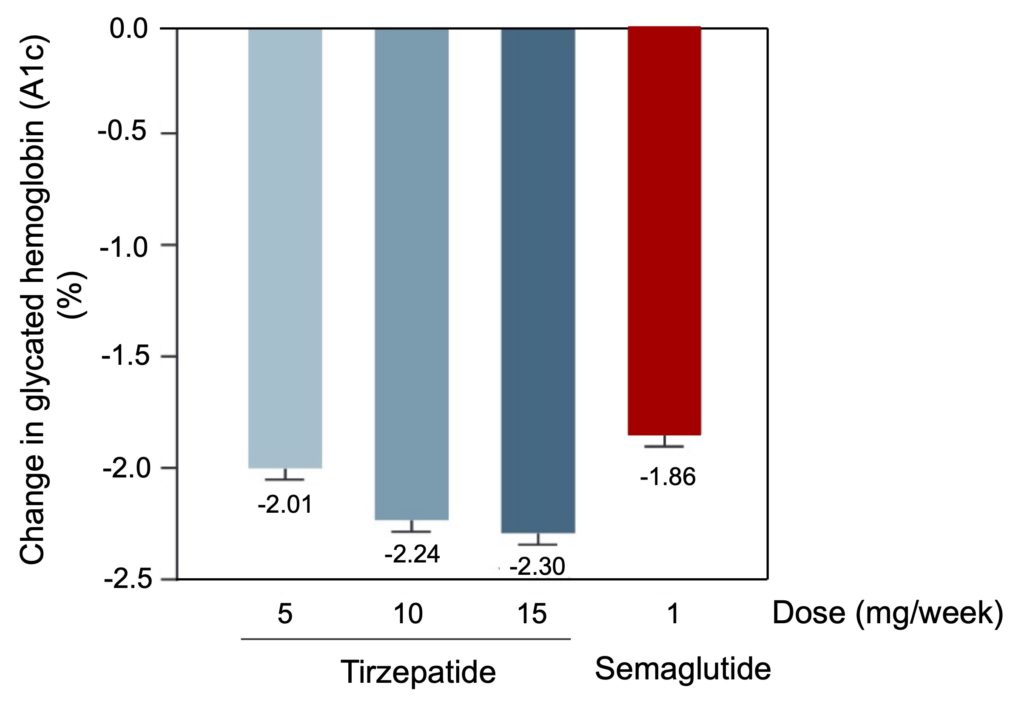
Figure 4. Comparison of the decrease in glycated hemoglobin levels of diabetic patients caused by a 40-week treatment with tirzepatide (5, 10 or 15 mg/wk) or semaglutide (1 mg/wk). Taken from Frias et al. (2021).
Effects on body weight
Another extremely interesting aspect of the mode of action of GLP-1 and GIP mimetics is their effect on certain processes involved in appetite control (Figure 3). In the GLP-1 infusion studies mentioned earlier, the molecule was observed to activate feelings of satiety, suggesting a possible therapeutic effect in decreasing appetite and caloric intake. Subsequent studies have shown that this phenomenon could be linked to a slowing of gastric emptying by GLP-1, as well as by the action of this hormone at the level of certain neural circuits of the brain involved in the suppression of appetite and the development of nausea. The action of GIP in the brain, however, also involves a decrease in appetite circuits but paradoxically would have an anti-nausea effect. This could explain why tirzepatide (which stimulates the GIP pathway in addition to GLP -1) can be administered at higher doses than semaglutide (which only stimulates GLP-1), without amplifying the side effects typical of GLP-1 agonists (nausea, vomiting).
Studies that have looked at the effects of semaglutide and tirzepatide on caloric intake confirm these impacts of both molecules on appetite. For example, in a study where obese volunteers had unlimited access (ad libitum) to three meals (lunch, dinner and snacks), it was observed that treatment with semaglutide (1 mg/wk) caused a 24% decrease in energy intake during the day, leading to a reduction in body weight of approximately 5 kg after 12 weeks of treatment. This reduction in calorie intake, and subsequent weight loss, is believed to be caused by a decrease in appetite and cravings and a reduction in cravings for high-fat foods. Similar results have been obtained following treatment with tirzepatide, and there is increasing evidence that decreased appetite and disinterest in high-calorie foods, particularly those high in fat,represents a common mode of action for both molecules.
A large number of clinical studies have shown that this loss of appetite caused by treatment with semaglutide or tirzepatide is associated with a significant decrease in body weight in people who suffer from obesity. For example, one study showed that in people with type 2 diabetes, treatment with semaglutide (1 mg weekly) causes an average loss of about 6% of body weight over 40 weeks, while treatment with tirzepatide (15 mg/week) leads to an 11% weight loss in this population.
These weight losses are even more pronounced in people who are obese but do not have diabetes (Figure 5). For example, administration of 2.4 mg/week of semaglutide (instead of 1 mg used in diabetics) for 68 weeks leads to average losses of 15% of initial body weight, approximately double that in type 2 diabetics (Figure 5A). Again, tirzepatide appears to be more potent, generating average losses of approximately 20% at the highest doses (10 and 15 mg/week) administered for 72 weeks (Figure 5B). These weight losses are truly exceptional, of the same order of magnitude as those typically obtained following bariatric surgery.
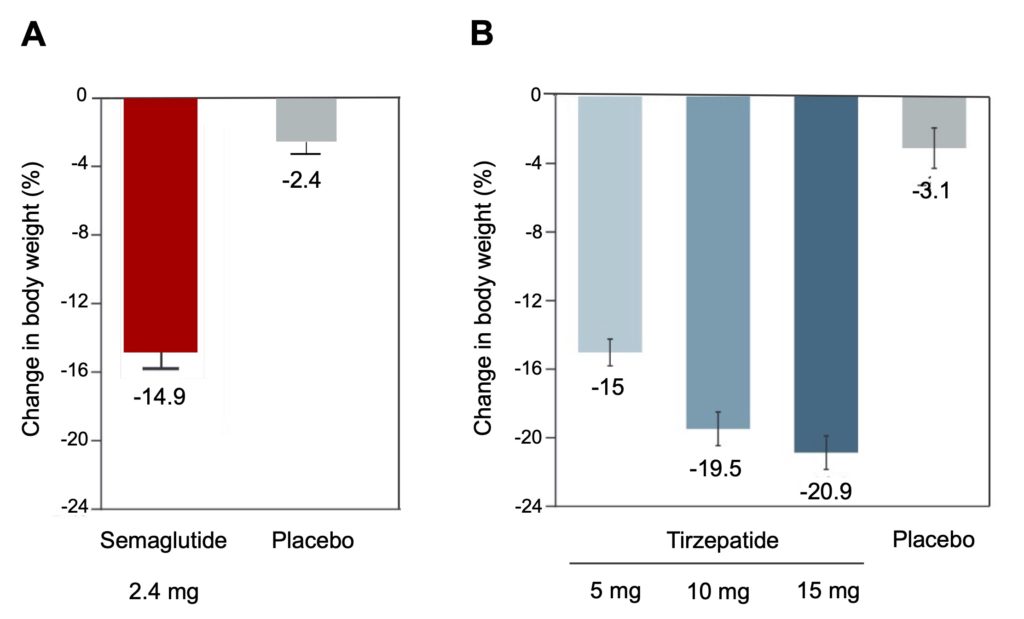
Figure 5. Mean weight loss induced by semaglutide and tirzepatide in obese but nondiabetic individuals. A. 1,961 obese adults (BMI>30) were treated for 68 weeks with placebo or 2.4 mg/week semaglutide, in combination with a supervised lifestyle improvement program (low-calorie diet and regular physical activity). Adapted from Wilding et al. (2021). B. 2,539 obese adults (BMI>30) were treated for 72 weeks with a placebo or doses of 5, 10 or 15 mg/week of tirzepatide, in combination with a supervised lifestyle improvement program (low-calorie diet and regular physical activity). Adapted from Jastreboff et al. (2022).
Several studies indicate that a sustained weight loss of at least 10% of initial body weight improves several complications associated with obesity, including the prevention and control of type 2 diabetes, hypertension, fatty liver disease and sleep apnea. For example, in the DiRECT study of people with obesity and diabetes, very severe caloric restriction leading to a loss of 15% of body weight led to complete remission of type 2 diabetes in 85% of participants.
Current data indicate that the vast majority of obese people treated with semaglutide and tirzepatide achieve weight losses of this magnitude (Figure 6). For example, semaglutide induces weight losses greater than 15% in 60% of those treated, and nearly 40% even lost more than 20% of their initial body weight (Figure 6A). These successes are even more pronounced in those treated with tirzepatide, with nearly 60% of patients losing 20% of their weight and nearly 40% losing even more than 25% of their initial weight (Figure 6B). These are considerable weight losses: in the 2 studies, the average weight of the participants was around 110 kg; a loss of 20% therefore means that these people have lost almost 25 kg during the treatment and it is certain that losses of this magnitude, if maintained in the long term, will have positive effects on health.
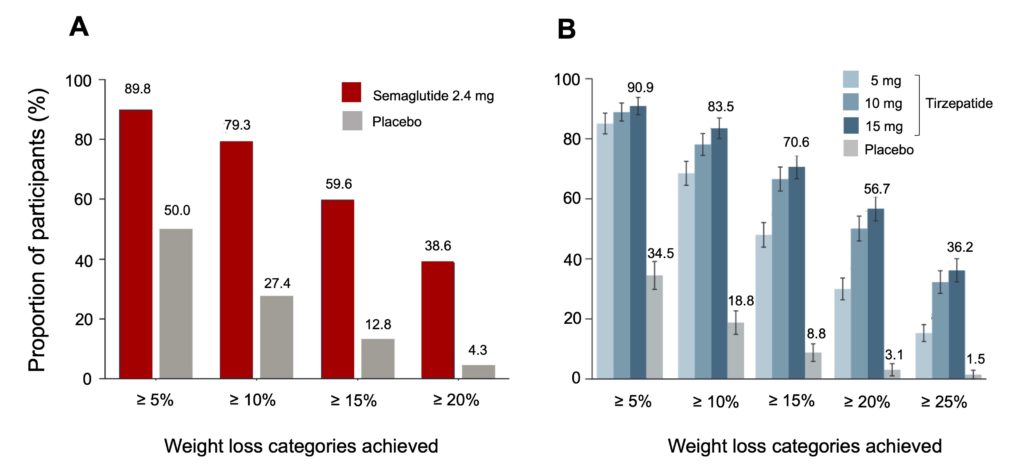
Figure 6. Distribution of weight loss according to the percentage of initial body weight lost following treatment.Note that in the majority of the participants, the weight loss obtained is well above 5% of the initial weight (the minimum associated with an improvement in health) and even exceeds 20% in many of them, in particular in the participants who received tirzepatide. For clarity, only the losses obtained for the highest dose of tirzepatide (15 mg) are shown in the figure. Adapted from Wadden et al. (2021) for semaglutide and Jastreboff et al. (2022) for tirzepatide.
Overall, these results unequivocally show that the decrease in appetite caused by GLP-1 and GIP mimetics is associated with a significant reduction in body weight. However, the data currently available suggests that continued treatment with these drugs is required for these weight losses to become sustainable. For example, one study showed that although people treated for 68 weeks with semaglutide (2.4 mg/week) lost an average of 18% of their initial body weight, the majority of this weight was regained within a year following discontinuation of treatment (Figure 7).
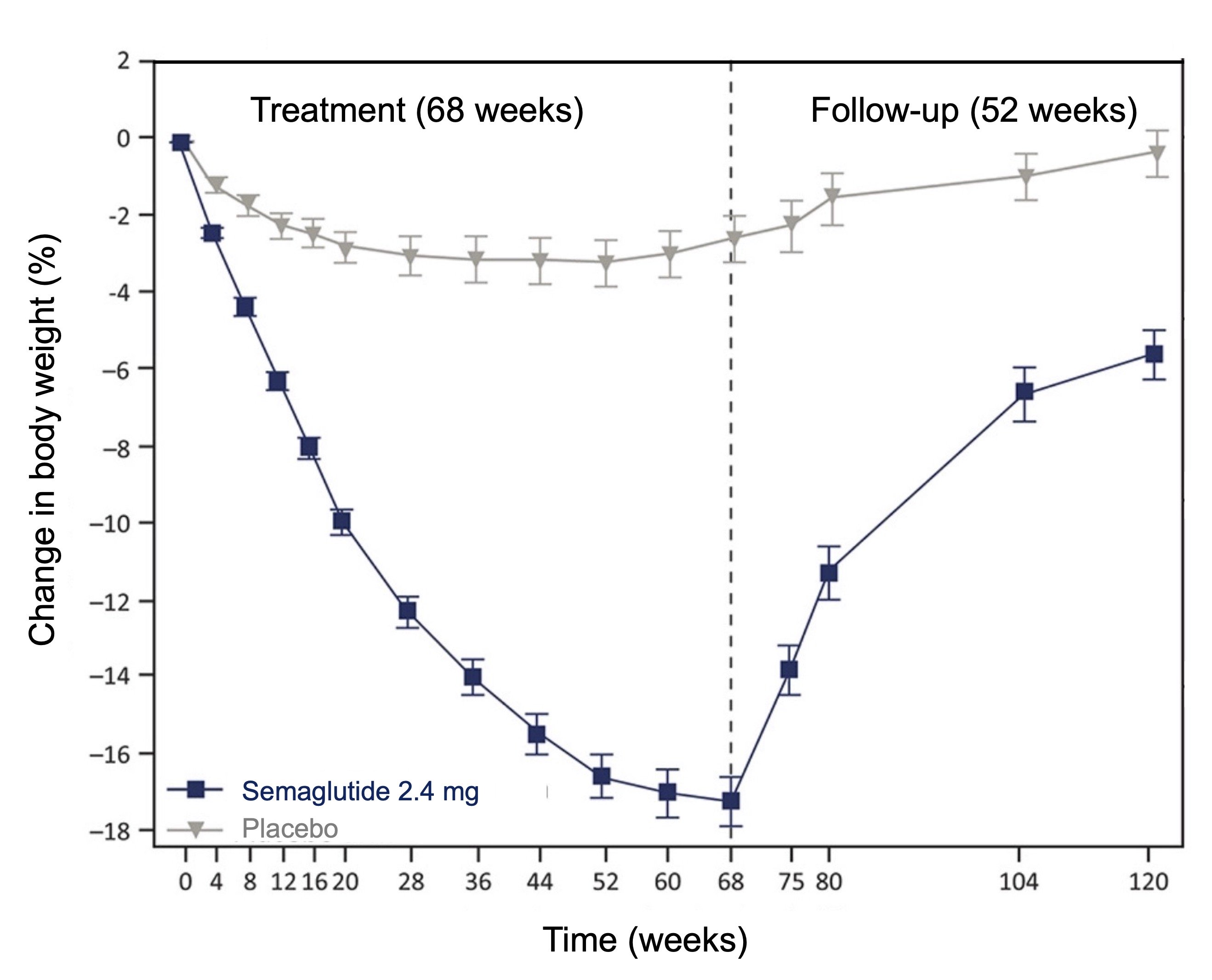
Figure 7. Reversibility of weight loss associated with treatment with semaglutide. Note that 2/3 of the weight lost by the participants was regained within a year of stopping treatment with semaglutide. Adapted from Wilding et al. (2022).
There is therefore no doubt that semaglutide and tirzepatide represent extremely interesting additions to the pharmacological approach to obesity, especially since these drugs are generally relatively well tolerated. Although a fairly large proportion of patients have reported a number of side effects, particularly at the gastrointestinal level (nausea, vomiting, diarrhoea), these side effects tend to diminish over time and adherence to treatment remains high, with about 5% of patients discontinuing treatment due to side effects.
From a more general point of view, it is particularly interesting that these drugs exert their therapeutic action by acting on the brain to reduce appetite and thus create a significant caloric deficit. This mode of action confirms what the experts have been saying for several years, namely that it is a reduction in calorie intake that remains the main means of losing weight (physical exercise has enormous health benefits, but does not have major effects on weight loss). The significant increase in the number of overweight people observed in recent decades therefore essentially reflects the overconsumption of food, possibly due to the omnipresence of industrial foods that are extremely attractive because of their organoleptic properties (palatability) and which lead to excessive energy intake. People treated with semaglutide and tirzepatide cease to be attracted to this type of high calorie food, and there is no doubt that the elimination of these products from the daily diet contributes to the weight losses observed in clinical studies.
However, currently available data indicate that this disinterest in high-calorie products (and overconsumption of food in general) is reversible and that stopping treatment quickly leads to a regain of most of the weight initially lost. It is therefore likely that these drugs will succeed in counteracting the physiological adaptations normally caused by weight loss (increased appetite, in particular), but that these adaptations quickly take over after stopping the medication and promote the return to the initial overweight, before treatment.
Does this mean that we have to resign ourselves to treating obesity “for life,” a bit like controlling hypertension, excess blood cholesterol or even insulin deficiency, with the help of drugs that should be administered continuously from the onset of pathologies? It is still too early to say, but, one thing is certain, such treatments would impose an extraordinary economic burden on our health care system. In Quebec, where one in four adults is obese, the current cost of these new drugs (approximately $500 per month) would involve an annual expenditure of several hundred million dollars (in the United States the situation is even worse: the cost of a 72-week course of tirzepatide (15 mg/week) is approximately US$17,000, while the 68-week treatment with semaglutide (2.4 mg/week) is nearly US$23,000!). As with all chronic diseases, it would be much more profitable to prevent obesity than to cure it by attacking the causes of this overweight as a priority, rather than devoting all our efforts and financial means to their treatment.
It has been known for several years that it is extremely difficult to lose weight once obesity has set in, which means that we must take a proactive approach with children and adolescents, before they accumulate excess weight that exposes them to a very high risk of obesity in adulthood (more than 80% of obese adults were already obese during their childhood). Unfortunately, the current trend is completely the opposite, with a steady increase in overweight and obesity affecting the youngest, putting them at very high risk of developing a veritable epidemic of cardiometabolic diseases in a few years (see our article on this subject). It is unrealistic to think that the arrival of new drugs alone will be able to curb this problem.