Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesOverview
- The Japanese have the highest life expectancy at birth among the G7 countries.
- The higher life expectancy of the Japanese is mainly due to fewer deaths from ischemic heart disease, including myocardial infarction, and cancer (especially breast and prostate).
- This exceptional longevity is explained by a low rate of obesity and a unique diet, characterized by a low consumption of red meat and a high consumption of fish and plant foods such as soybeans and tea.
Several diets are conducive to the maintenance of good health and to the prevention of cardiovascular disease, for example, the Mediterranean diet, the DASH diet (Dietary Approaches to Stop Hypertension), the vegetarian diet, and the Japanese diet. We often refer to the Mediterranean Diet in these pages, because it is well established scientifically that this diet is particularly beneficial for cardiovascular health. Knowing that the Japanese have the highest life expectancy among the G7 countries, the special diet in Japan has also captured the attention of experts and an informed public in recent years.
Japanese life expectancy
Among the G7 countries, Japan has the highest life expectancy at birth according to 2016 OECD data, particularly for women. Japanese men have a slightly higher life expectancy (81.1 years) than that of Canadian men (80.9 years), while the life expectancy of Japanese women (87.1 years) is significantly higher (2.4 years) than that of Canadian women (84.7 years). The healthy life expectancy of the Japanese, 74.8 years, is also higher than in Canada (73.2 years).
The higher life expectancy of Japanese people is mainly due to fewer deaths from ischemic heart disease and cancers, particularly breast and prostate cancer. This low mortality is mainly attributable to a low rate of obesity, low consumption of red meat, and high consumption of fish and plant foods such as soybeans and tea. In Japan, the obesity rate is low (4.8% for men and 3.7% for women). By comparison, in Canada 24.6% of adult men and 26.2% of adult women were obese (BMI ≥ 30) in 2016. Obesity is an important risk factor for both ischemic heart disease and several types of cancers.
Yet in the early 1960s, Japanese life expectancy was the lowest of any G7 country, mainly due to high mortality from cerebrovascular disease and stomach cancer. The decrease in salt and salty food intake is partly responsible for the decrease in mortality from cerebrovascular disease and stomach cancer. The Japanese consumed an average of 14.5 g of salt/day in 1973 and probably more before that. They eat less salt these days (9.5 g/day in 2017), but it’s still too much. Canadians now consume on average about 7 g of salt/day (2.76 g of sodium/day), almost double the intake recommended by Health Canada.
The Japanese diet
Compared to Canadians, the French, Italians and Americans, the Japanese consume much less meat (especially beef), dairy products, sugar and sweeteners, fruits and potatoes, but much more fish and seafood, rice, soybeans and tea (Table 1). In 2017, the Japanese consumed an average of 2,697 kilocalories per day according to the FAO, significantly less than in Canada (3492 kcal per day), France (3558 kcal per day), Italy (3522 kcal per day), and the United States (3766 kcal per day).
Table 1. Food supply quantity (kg/capita/year) in selected countries in 2013a.
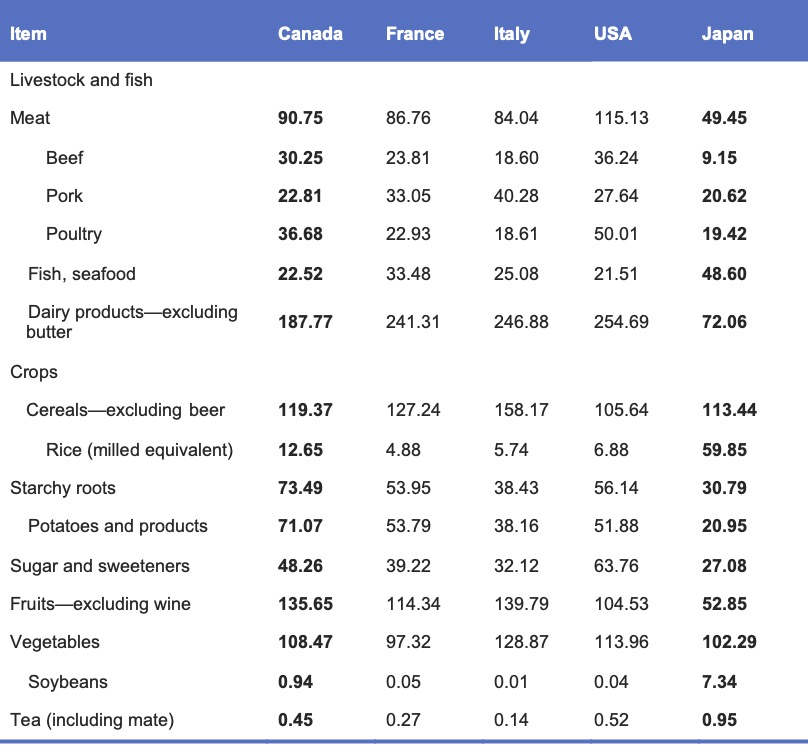
aAdapted from Tsugane, 2020. FAO data: FAOSTAT (Food and agriculture data) (http://www.fao.org/).
Less red meat, more fish and seafood
The Japanese eat on average almost half as much meat as Canadians (46% less), but twice as much fish and seafood. This considerable difference translates into a reduced dietary intake of saturated fatty acids, which is associated with a lower risk of ischemic heart disease, but an increased risk of stroke. On the contrary, dietary intake of omega-3 fatty acids found in fish and seafood is associated with a reduced risk of ischemic heart disease. The lower consumption of red meat and higher consumption of fish and seafood by the Japanese could therefore explain the lower mortality from ischemic heart disease and the higher mortality from cerebrovascular disease in Japan. Experts believe that the decline in death from cerebrovascular disease is associated with changes in the Japanese diet, specifically increased consumption of animal products and dairy products, and consequently of saturated fat and calcium (a consumption which remains moderate), combined with a decrease in salt consumption. Indeed, contrary to what is observed in the West, the consumption of saturated fat in Japan is associated with a reduction in the risk of hemorrhagic stroke and to a lesser extent of ischemic stroke, according to a meta-analysis of prospective studies. The cause of this difference is not known, but it could be attributable to genetic susceptibility or confounding factors according to the authors of the meta-analysis.
Soybeans
Soy is a food mainly consumed in Asia, including Japan where it is consumed as is after cooking (edamame) and especially in processed form, by fermentation (soy sauce, miso paste, nattō) or by coagulation of soy milk (tofu). It is an important source of isoflavones, molecules that have anticancer properties and are beneficial for good cardiovascular health. Consumption of isoflavones by Asians has been linked to a lower risk of breast and prostate cancer (see our article on the subject).
Sugar
The Japanese consume relatively few sugars and starches, which partly explains the low prevalence of obesity-associated diseases such as ischemic heart disease and breast cancer.
Green tea
The Japanese generally consume green tea with no added sugar. Prospective studies from Japan show that green tea consumption is associated with a lower risk of all-cause mortality and cardiac death.
Westernization of Japanese eating habits
The westernization of the Japanese diet after World War II allowed the inhabitants of this country to be healthier and to reduce mortality caused by infectious diseases, pneumonia and cerebrovascular diseases, thereby considerably increasing their life expectancy. A survey of the eating habits of 88,527 Japanese from 2003 to 2015 indicates that this westernization continues. Based on the daily consumption of 31 food groups, the researchers identified three main types of eating habits:
1- Plant foods and fish
High intakes of vegetables, fruits, legumes, potatoes, mushrooms, seaweed, pickled vegetables, rice, fish, sugar, salt-based seasonings and tea.
2- Bread and dairy
High intakes of bread, dairy products, fruits and sugar. Low intake of rice.
3- Animal foods and oils
High intakes of red and processed meat, eggs, vegetable oils.
A downward trend in the “plant foods and fish” group (the staple of the traditional Japanese diet or washoku) was observed in all age groups. An increase in the “bread and dairy” group was observed in the 50–64 and ≥65 years age groups, but not among the youngest. For the “animal foods and oils” group, an increasing trend was observed during the thirteen years of the study in all age groups except the youngest (20–34 years). The Japanese are eating more and more like Westerners. Will this have an adverse effect on their health and life expectancy? It is too early to know, only the next few decades will tell.
Contribution of genes and lifestyle to the health of the Japanese
Some risk factors for cardiovascular disease and cancer are hereditary, while others are associated with lifestyle (diet, smoking, exercise, etc.). At the turn of the 20th century, there was significant Japanese immigration to the United States (especially California and Hawaii) and South America (Brazil, Peru). After a few generations, the descendants of Japanese migrants adopted the way of life of the host countries. While Japan has one of the lowest incidences of cardiovascular disease in the world, this incidence doubled among the Japanese who migrated to Hawaii and quadrupled among those who chose to live in California according to a 1975 study. What is surprising is that this increase has been observed regardless of blood pressure or cholesterol levels, and seems rather directly related to the abandonment of the traditional Japanese way of life by migrants.
Since the 1970s, the average cholesterol level of the Japanese has nonetheless increased, but despite this and the high rate of smoking in this country, the incidence of coronary heart disease remains substantially lower in Japan than in the West. To better understand these differences, a 2003 study compared the risk factors and diets of Japanese living in Japan with third- and fourth-generation Japanese migrants living in Hawaii in the United States. Men’s blood pressure was significantly higher among Japanese than among Japanese-Americans, while there was no significant difference for women. Far fewer Japanese were treated for hypertension than in Hawaii. More Japanese people (especially men) smoked than Japanese-Americans. Body mass index, blood levels of LDL cholesterol, total cholesterol, glycated hemoglobin (an indicator for diabetes), and fibrinogen (a marker of inflammation) were significantly lower in Japan than in Hawaii. HDL cholesterol (the “good” cholesterol) was higher in the Japanese than in the Japanese-Americans. The dietary intake of total fat and saturated fatty acids (harmful to cardiovascular health) was lower in Japan than in Hawaii. In contrast, the intake of polyunsaturated fatty acids and omega-3 fatty acids (beneficial for good cardiovascular health) was higher in Japan than in Hawaii. These differences may partly explain the lower incidence of coronary heart disease in Japan than in Western industrialized countries.
In other words, even if these migrants have the same basic risk as their compatriots who have remained in the country of origin (age, sex and heredity), the simple fact of adopting the lifestyle of their host country is enough to significantly increase their risk of cardiovascular disease.
Although the Japanese diet is different from those of Western countries, it has similar characteristics to the Mediterranean diet. Why not prepare delicious Japanese soy dishes from time to time (for example, tofu, edamame, miso soup), drink green tea, eat less meat, sugar and starch and more fish? Not only will your meals be more varied, but you could enjoy the health benefits of the Japanese diet.