Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesUpdated on September 11, 2018
The dramatic increase in population body weight over the past 40 years is becoming the major public health problem of our generation. Once a very rare phenomenon, the prevalence of obesity is rising sharply in most countries worldwide, reaching 5% among children (108 million) and 12% among adults (604 million) in 2015. In Canada, the situation is even worse, with no less than 62% of the adult population being overweight, including 27% who are obese. Moreover, this is not improving, as we are also among the top countries with the highest rates of overweight children and adolescents, with 15% of young boys and 10% of young girls who are obese.
These statistics are truly alarming, as overweight, and more specifically obesity, is an important risk factor for a wide range of chronic diseases, including cardiovascular disease, type 2 diabetes, at least 13 types of cancer, and various musculoskeletal disorders. The negative impacts of having an overweight population are already beginning to appear: in the United States, where the prevalence of obesity is one of the highest in the world, a report by the Center for Disease Control and Prevention (CDC) recently showed a decrease in life expectancy due in part to the effects of obesity on cardiovascular disease. In other words, the dramatic increase in the number of overweight people is counteracting the benefits of decreased tobacco use in recent years, with disastrous consequences for both the population’s life expectancy and quality.
Losing weight is hard
Overweight is basically the result of an imbalance caused by the consumption of calories in excess of the body’s energy needs. In theory, the treatment of obesity is therefore relatively simple: it is a matter of restoring a balance between caloric intake and expenditure, for example by eating less and moving more, which causes an energy deficit that leads over time to the dissipation of excess calories accumulated in the form of fat, and, therefore, to weight loss.
In reality, losing weight, and especially maintaining weight loss in the long term, is an extremely difficult task that the majority of overweight people are unable to successfully achieve. For example, in a randomized study on the impact of four popular diets (Atkins, Zone, Weight Watchers and Ornish), researchers noted that the weight loss achieved by each of these diets was relatively modest (in the order of 2-3 kg), a failure that can be explained in large part by the very high attrition rate among participants. Greater weight loss, in the order of 20 kg, can be achieved in the short term with even more severely calorie-deficient diets, but again, adherence to these extreme diets is very low, and weight loss is quickly followed by weight gain. This is a major problem, as obesity is a chronic condition that requires sustained weight loss over a long period of time to significantly reduce the risk of developing the range of problems resulting from being overweight.
This difficulty in losing weight is due to the fact that caloric intake and caloric expenditure are interrelated phenomena that exert a mutual influence in order to maintain a stable body weight. In practical terms, this means that changes in energy balance, whether due to decreased caloric intake and/or increased physical activity levels, are countered by a series of physiological adaptations that resist weight loss, for example by decreasing basal metabolic rate. As a result, even if a person manages to create an energy deficit by eating less or being more active, it is usually offset by a corresponding decrease in the energy expended by the body or by an increase in appetite to compensate for missing calories. The difficulty in losing weight is therefore not due to a lack of willpower, as still too many people think, but rather a consequence of our metabolism’s fierce resistance to anything that is likely to cause weight loss.
Low-carbohydrate diets
In recent years, it has been proposed that low-carbohydrate but high-fat diets (“low-carb, high-fat”, or LCHF) may be a solution to bypass the body’s “defense” mechanisms and increase weight loss (see box for a summary of the scientific aspects of this approach). Since carbohydrates cause a marked increase in insulin levels, which is the hormone involved in the conservation of energy stored in the form of fat, it is proposed that a low-carbohydrate diet could reduce insulin levels, thus allowing the body to mobilize fat stored in adipose tissue and to use it as a source of energy. According to the model, this increased use of fat would result in an increase in metabolism (around 500 kcal/day), and should therefore allow significant weight loss.
In Canada, the food guide recommends consuming about 300 g of carbohydrates per day, which corresponds to 1,200 calories, or 60% of the total calorie consumption of an average adult (2,000 calories). In a low-carbohydrate diet, this proportion is around 20% of total calories (100 g of carbohydrates) and can even decrease to 5% of calories (20 g of carbohydrates, equivalent to a single slice of bread) in ketogenic diets.
The principle behind low-carb diets is that calories from carbohydrates favour more accumulation of excess weight than calories from fat. In other words, it is not so much the quantity, but especially the type of calories consumed that are important for weight loss. This hypothesis is based on two well-documented effects of insulin on metabolism:
1) In carbohydrate-rich diets, the insulin secreted by the pancreas allows fat cells to capture the sugars released into the blood and to turn them into fat for future use.
2) Simultaneously, insulin blocks the use of calories accumulated in fat tissue, thus preventing weight loss. These actions of insulin ensure that fat tissue not only accumulates excess calories, but that these calories cannot even be used to support the body’s energy needs.
In other words, even if there is a surplus of stored energy, the body is in famine mode! In response to this deficiency, it reduces its basal metabolic rate to save energy (which helps prevent the use of excess calories) and simultaneously increases appetite to obtain the calories needed to maintain these functions. There is therefore a vicious circle in which excess carbohydrates lead to overweight, and overweight leads to an increase in food consumption. This model would explain the increase in body weight observed in a large number of people with diabetes who are treated with insulin.
The impact of low-carb diets on body weight has been the subject of a very large number of randomized clinical studies over the past two decades. In general, these studies show that in the short term (3 to 6 months), obese or morbidly obese people experience significant weight loss on these diets compared to traditional low-calorie diets (low-fat diets, for example). In most cases, however, weight loss is temporary and decreases considerably over time: the difference in kilos lost 2 years into various diets is minimal and insufficient to have a significant clinical impact (Figure 1).
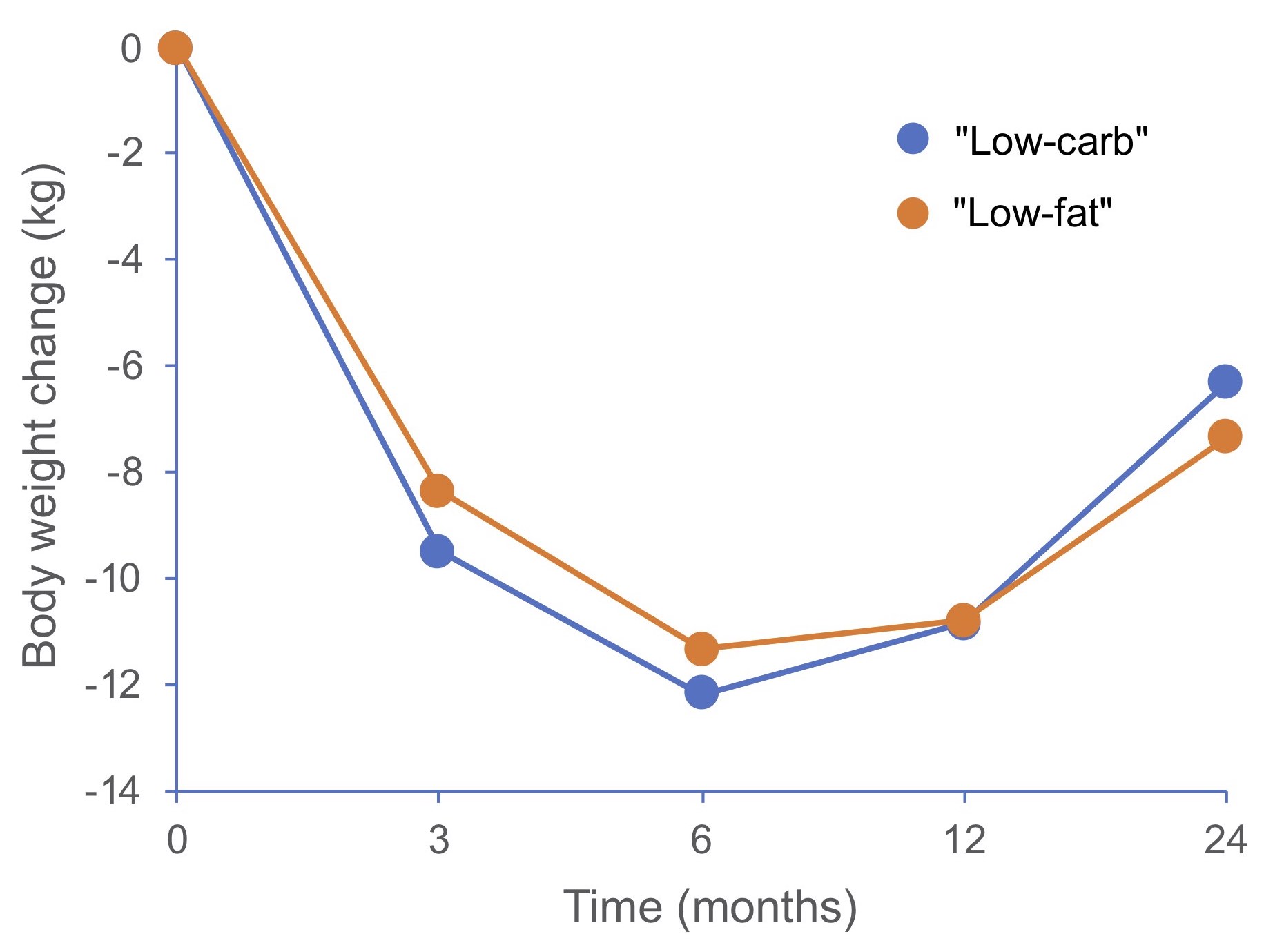
Figure 1. Comparison of the weight loss achieved with low-carbohydrate or low-fat diets over a 2-year period. Adapted from Foster (2010).
Several meta-analyses of randomized clinical trials comparing weight loss for low-fat and low-carb diets confirm the slight advantage of low-carb diets, but show that additional weight loss from these diets is relatively modest, at around 1-2 kg (Table 1).
Table 1. Summary of meta-analyses comparing weight loss obtained with low-carbohydrate (low-carb) or low-fat diets.
| Meta-analyses | Number of randomized studies included | Total number of participants | Diet with highest fat loss | Additional weight loss (kg) |
|---|---|---|---|---|
| Nordmann et al. (2006) | 5 | 447 | Low-carb | 1.0 |
| Hession et al. (2009) | 7 | 1222 | Low-carb | 1.05 |
| Bueno et al. (2013) | 13 | 1415 | Low-carb | 0.91 |
| Tobias et al. (2015) | 18 | 2736 | Low-carb | 1.15 |
| Sackner-Bernstein et al. (2015) | 17 | 1797 | Low-carb | 2.04 |
| Mansoor et al. (2016) | 11 | 1369 | Low-carb | 2.17 |
| Meng et al. (2017) | 8 | 734 | Low-carb | 0.94 |
To explain these disappointing results, it should first be mentioned that the theory on which low-carb diets are based, i.e., a decrease in insulin increases the body’s energy expenditure and fat metabolism, seems inaccurate. When researchers rigorously measured energy expenditure in response to diets containing either low amounts of fat or carbohydrates, they observed that the increase in metabolism from low-carb diets is very low and has no major impact on weight loss. In fact, the opposite is true: for equal calories, weight loss is slightly higher for people on a low-fat diet compared to a low-carbohydrate diet.
Hence, there does not seem to be any major advantage to preferentially restricting carbohydrate intake to promote weight loss. Although sometimes significant, the weight loss that occurs in the first few months of these diets tends to diminish over time, becoming similar to results obtained for low-calorie diets. The most important factor is limiting total calories, whether from carbohydrates or fat. In fact, studies show that people who diligently follow low-calorie diets for at least 2 years manage to achieve significant weight loss, whether or not these diets are rich in carbohydrates, fats or proteins.
Impact on cardiovascular health
Several studies have examined the impact of low-carb diets on cardiovascular risk factors and, again, the results do not seem to show significant advantages over conventional low-calorie diets. In the short term, studies indicate that low-carb diets increase HDL cholesterol levels and decrease triglycerides, which is positive, but simultaneously increase LDL cholesterol levels (due to a higher intake of saturated fat), which is negative. However, since these effects disappear over time, they likely do not have major clinical implications. It should be noted that the increase in HDL cholesterol levels observed in response to low-carb diets is maintained over the longer term and remains about twice as high as for people on a low-fat diet. An increase in HDL levels is generally considered beneficial to cardiovascular health, but its real impact in a context where saturated fat intake is high (as with low-carb diets) is yet to be established. Overall, it can be argued that weight loss is the most important factor in improving the cardiovascular health of people who are obese, regardless of the diet used.
Inter-individual variations
It is important to note that the results of the studies mentioned here indicate the average weight loss observed in a population on a given weight loss diet. However, in each of these groups, there are major differences in the response to these diets, with some people losing a lot of weight, others losing less, and some even gaining weight. This phenomenon is observed for all diets, whether they are low in carbohydrates or fat (Figure 2).
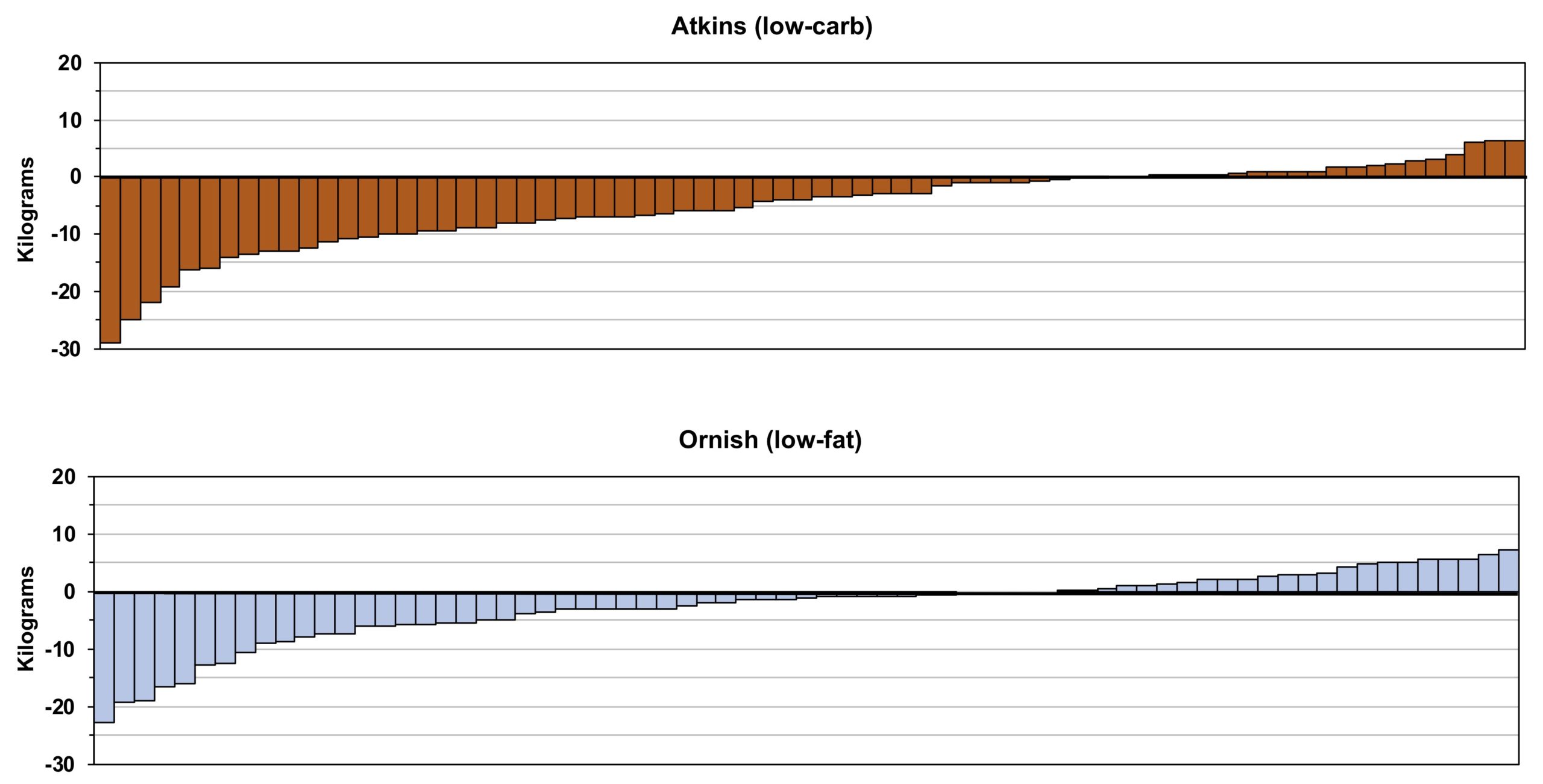
Figure 2. Distribution of weight changes for each participant in a study comparing the effectiveness of low-carbohydrate (Atkins) and low-fat (Ornish) diets. Adapted from Gardner (2012).
All of the factors responsible for these significant variations are not yet known, but they likely reflect the heterogeneity of the human metabolism and its very different responses to food. For example, it is known that postprandial glucose responses (a risk factor for cardiovascular disease and premature death) vary considerably from person to person, even when they eat exactly the same meal. A host of factors have been proposed to explain this phenomenon (sleep-wake cycle, mealtime, level of physical activity, composition of the intestinal microbiome), but the degree of insulin sensitivity is certainly among the most important. Several studies have reported that insulin-resistant (diabetic and prediabetic) people lose more weight on a low-carbohydrate diet than on a low-fat diet, whereas, conversely, low-fat diets may work better for people with greater insulin sensitivity. The advantages of a low-carb diet in this population do not seem to be limited to weight loss: a recent study showed that compared to a low-fat diet, a low-carb diet with mainly unsaturated fat resulted in a greater improvement in lipid profile and blood sugar levels, and a reduction in medication in obese and diabetic patients, despite similar weight loss. Low-carbohydrate diets may therefore be a promising approach for the optimal treatment of type 2 diabetes.
It is also possible that a low-carbohydrate diet may have additional positive effects. For example, it has been suggested that the high consumption of carbohydrate-rich foods preferentially increases the accumulation of fat in the viscera and liver, which in turn increases the risk of cardiovascular disease and type 2 diabetes. It has also been suggested that a very low-carbohydrate diet could reduce appetite by increasing blood ketone levels. Low-carb diets are also often associated with higher protein consumption, which could contribute to an increased sense of satiety, thus lowering total caloric intake.
In short, there is no universal solution to weight loss, and low-carbohydrate diets can be an interesting tool to help some people lose weight. One advantage of these diets is the elimination of sources of simple sugars (sweets, soft drinks, foods made with refined flour), which do not provide any useful benefits for health and are known to promote overweight and the development of several chronic diseases. However, a major disadvantage is that these diets limit the intake of certain plant-based foods known to have very positive impacts on the prevention of cardiovascular disease and overall health, such as fruits, legumes and whole grain products.
Another negative aspect of low-carb diets is that they often recommend a high intake of saturated animal fats (red meat, cured meats, dairy products), which increase LDL cholesterol levels, an important risk factor for cardiovascular disease. Recent results indicate that this type of diet can be harmful to health: for example, one study showed that people whose carbohydrate intake was less than 40% of total calories had a 20% higher risk of premature death than those whose carbohydrate intake was 50-55% of total calories. However, this increased risk is only observed in people who replace carbohydrates with animal proteins and fats; when carbohydrates are replaced by foods of plant origin, on the contrary, there is a decrease (18%) in the risk of premature death.
These observations are consistent with several studies showing that the substitution of saturated fat with unsaturated fat is associated with a marked decrease in the risk of cardiovascular events and mortality (Figure 3). People who wish to adopt a low-carb approach are therefore well advised to limit the consumption of saturated fats and instead turn to polyunsaturated fats (avocados, fatty fish, nuts, flaxseed, etc.) as a primary source, due to the well-documented cardioprotective effect of these fats.
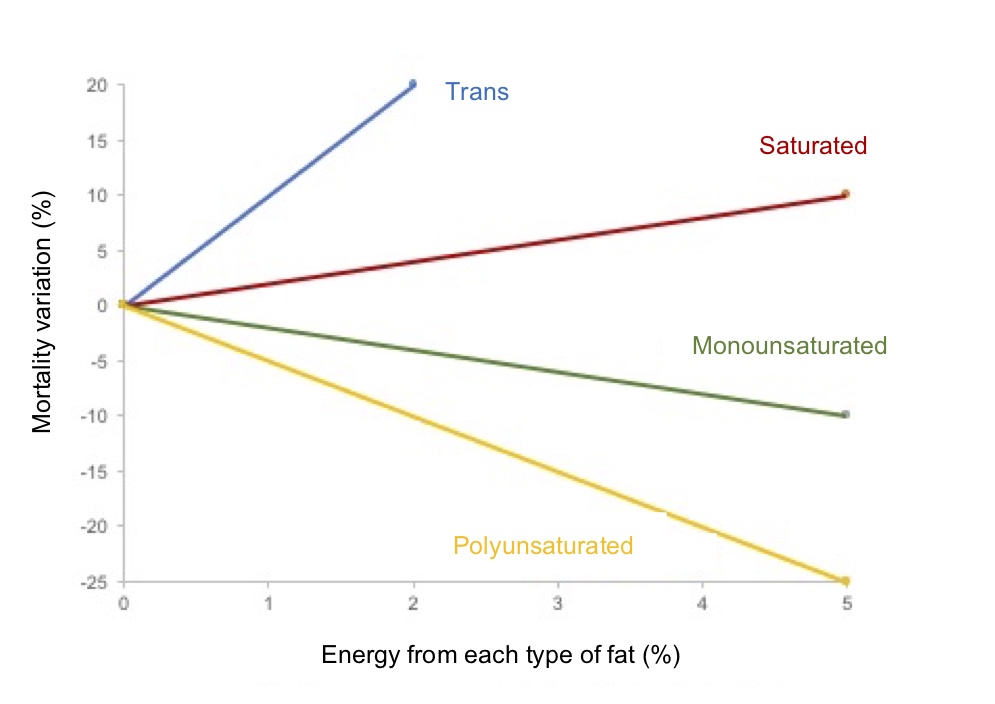
Figure 3. Variation in the risk of premature mortality according to the proportion of different types of fat in the diet. Adapted from Wang et al. JAMA Intern. Med. 2016; 176: 1134-1145.