Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesOverview
- Periodontitis is an inflammatory reaction affecting the periodontium, i.e., all the structures responsible for anchoring the teeth (gums, ligaments, alveolar bone).
- A very large number of studies have observed a close link between periodontitis and an increased risk of several pathologies, including myocardial infarction and stroke.
- The expansion of health insurance to cover dental care would therefore be an important step forward for cardiovascular prevention and the prevention of several other chronic diseases.
It is now clearly established that the microbiome, the vast bacterial community that lives in symbiosis with us, plays an essential role in the functioning of the human body and the maintenance of good health. This link is particularly well documented with regard to the intestinal microbiome, that is, the hundreds of billions of bacteria that are located in the digestive system, in particular at the level of the colon. In recent years, an impressive number of studies have shown that these bacteria play a leading role in the proper functioning of the metabolism and the immune system and that imbalances in the composition of the microbiome are associated with the development of several chronic diseases.
Oral microbiome
The mouth represents another privileged site of colonization by bacteria; each mL of saliva from a healthy adult contains approximately 100 million bacterial cells, not to mention the millions of bacteria present in other areas of the oral cavity, such as dental plaque, tongue, cheeks, palate, throat and tonsils. It is therefore not surprising that a simple 10-second kiss with tongue contact and exchange of saliva (French kiss) can transfer around 80 million bacteria between partners!
On average, the human mouth contains about 250 distinct bacterial species, from the approximately 700 species of oral bacteria that have been identified so far. The composition of this bacterial community is unique to each person and is influenced by their genetics, age, place of residence, cohabitation with other people, the nature of the diet and, obviously, the frequency of oral hygiene care.
In a healthy mouth, the oral bacterial community is a balanced ecosystem that performs several beneficial functions for the host. For example, some bacteria have anti-inflammatory activity that can block the action of certain pathogens, while others reduce the acidity of dental plaque (through the production of basic compounds such as ammonia) and thus prevent the demineralization of teeth, the first step in the process of tooth decay. Oral bacteria also have the ability to convert nitrates found in fruits and vegetables into nitric oxide (NO), a vasodilator that helps control blood pressure (see our article on this subject).
Disturbed ecosystem
It is the disruption of this balance of the bacterial ecosystem (dysbiosis) that is the trigger for the two main diseases affecting the teeth, namely dental caries and periodontal disease. In the case of caries, the cause is the establishment of a bacterial community enriched in certain species (Streptococci of the mutans group, in particular), capable of fermenting dietary sugars and reducing the pH sufficiently to initiate the demineralization of the tooth. The action of these bacteria is however local, restricted to the level of tooth enamel, and therefore generally does not have a major impact on health in general.
The global repercussions associated with periodontal diseases are much more serious, and it is for this reason that these infections have attracted a great deal of interest from the scientific and medical communities in recent years. Not only with regard to the identification of the bacteria responsible for these infections and their mechanisms of action, but also, and perhaps above all, because of the close relationship observed in several epidemiological studies between periodontitis and several serious chronic diseases, including cardiovascular disease, diabetes, certain cancers and even Alzheimer’s disease.
Periodontitis
As its name suggests, periodontitis is an inflammatory reaction affecting the periodontium, i.e., all the structures responsible for anchoring the teeth (gums, ligaments, alveolar bone) (Figure 1). Periodontitis begins in the form of gingivitis, which is local inflammation of the gums caused by bacteria present in dental plaque (the bacterial biofilm that forms on the teeth). This inflammation is usually quite benign and reversible, but can progress to chronic periodontitis in some more susceptible individuals. There is then a gradual resorption of the gums, ligaments and alveolar bone, which causes the appearance of periodontal pockets around the tooth and, eventually, its fall. Periodontal disease is one of the most common chronic inflammatory diseases, affecting almost 50% of the population to varying degrees, including 10% who develop severe forms of the disease, and is one of the main causes of tooth loss.
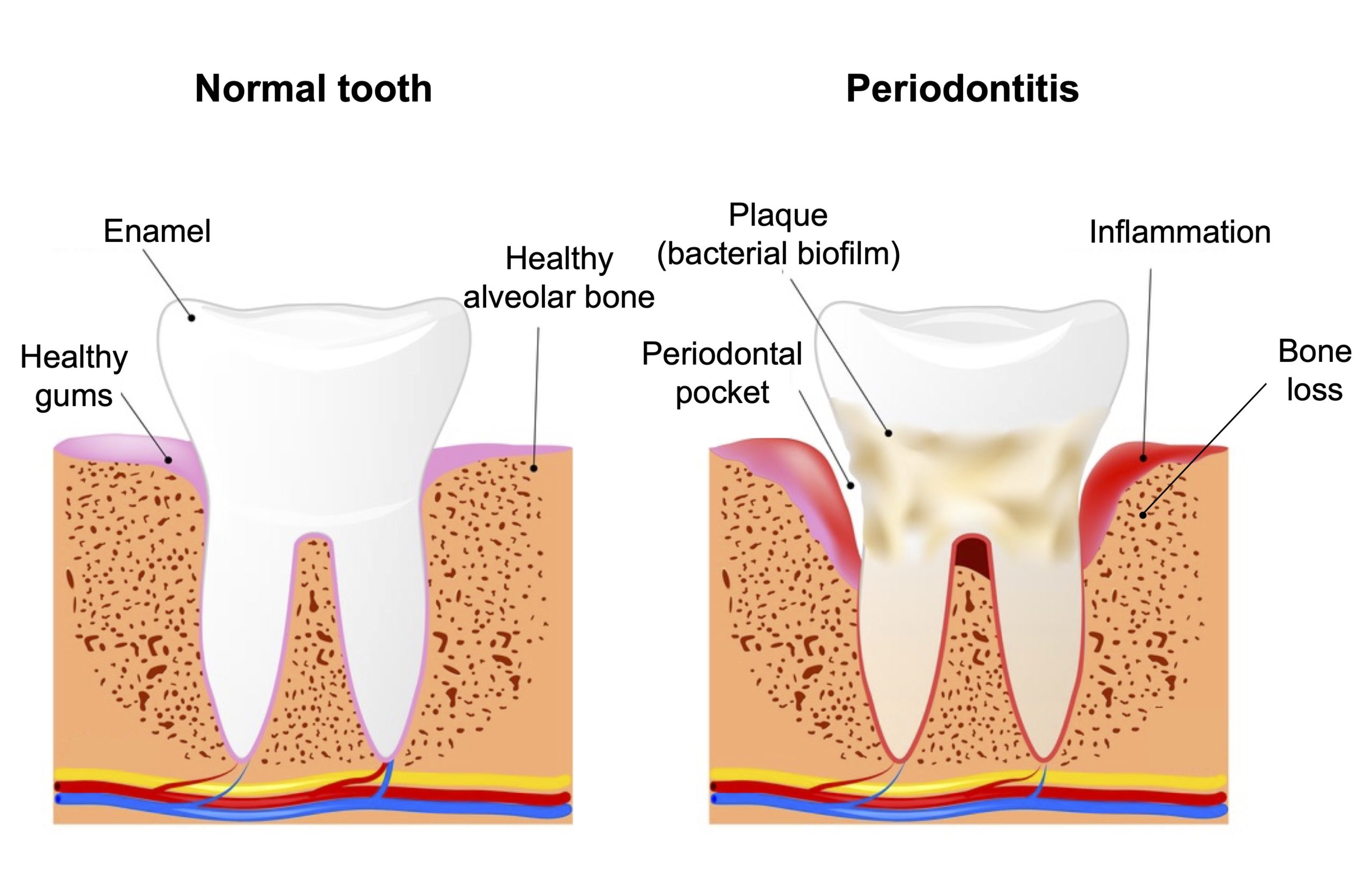
Figure 1. Schematic illustration of the main features of periodontitis. Image from Shutterstock.
The trigger factor for periodontitis is an imbalance in the composition of the microbial community present in dental plaque that promotes the growth of pathogenic species responsible for this infection. Among the approximately 400 different species of bacteria associated with dental plaque, the presence of a complex composed of the anaerobic bacteria Porphyromonas gingivalis, Treponema denticola, and Tanneralla forsythia (known as the red complex) is closely correlated with clinical measures of periodontitis, and more particularly with advanced periodontal lesions, and could therefore play an important role in the development of these pathologies. It is also interesting to note that the analysis of human skeletons has revealed that periodontitis became more frequent around 10,000 years ago (in the Neolithic period) and that this increase coincides with the increased presence of one of these bacteria (P. gingivalis) in dental plaque. It is likely that this change in plaque microbial composition is a consequence of changes in the human diet introduced by agriculture, in particular a higher carbohydrate intake.
A disproportionate inflammatory response
It is the exaggerated inflammatory response caused by the presence of this bacterial imbalance in dental plaque that is largely responsible for the development of periodontitis (Figure 2).
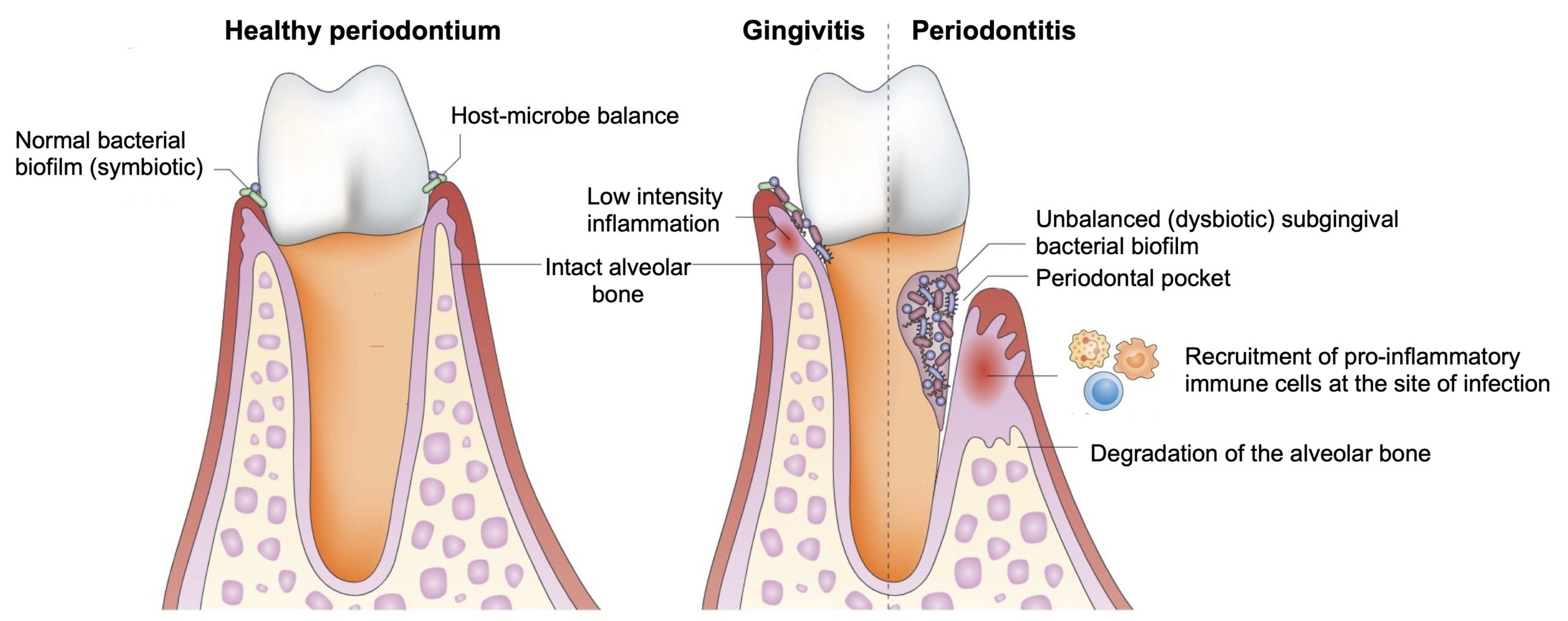
Figure 2. Impact of inflammation generated by bacterial imbalance (dysbiosis) on the development of periodontitis. In a healthy mouth (left figure), the bacterial biofilm is in balance with the host’s immune system and does not generate an inflammatory response. Disruption of this balance (by poor dental hygiene or smoking, for example) can cause gingivitis, which is a mild inflammation of the gums characterized by the formation of a slight gingival crevice (≤ 3 mm deep), but without bone damage. Gingivitis can progress to periodontitis when the bacterial imbalance of the biofilm induces a strong inflammatory reaction that destroys the tissues surrounding the tooth to form deeper periodontal pockets (≥ 4 mm) and the destruction of the alveolar bone. From Hajishengallis (2015).
When they manage to colonize the subgingival space, pathogenic bacteria such as P. gingivalis secrete numerous virulence factors (proteases, hemolytic factors, etc.) that degrade the tissues present at the site of infection and generate the essential elements for the growth of these bacteria. The bleeding gums caused by this infection is particularly beneficial for P. gingivalis since the growth of this bacterium requires a high supply of iron, present in the heme group of the hemoglobin of red blood cells.
The immune system obviously reacts strongly to this microbial invasion (which can reach several hundred million bacteria in certain deep periodontal pockets) by recruiting at the site of infection the first-line innate immunity (neutrophils, macrophages), specialized in the rapid response to the presence of pathogens. There is then massive production of cytokines, prostaglandins, and matrix metalloproteinases by these immune cells which, collectively, create a high-intensity inflammation intended to eliminate the bacteria present in the periodontal tissues.
However, this inflammatory response does not have the expected effects at all. On the one hand, periodontal bacteria have developed several subterfuges to escape the immune response and are therefore little affected by the host response; on the other hand, the continuous presence of an inflammatory microenvironment causes considerable damage to the periodontal tissues, which accelerates their destruction and the resorption of the gums, ligaments and bone characteristic of periodontitis. This inflammatory attack on the periodontium also has the perverse effect of generating several essential nutrients for bacterial growth, which further amplifies the infection and accelerates the degradation of the tissues surrounding the tooth. In other words, periodontitis is the result of a vicious circle in which the bacterial imbalance associated with dental plaque provokes a strong inflammatory immune response, with this inflammation leading to the destruction of the periodontal tissues, which in turn promotes the growth of these bacteria (Figure 3).
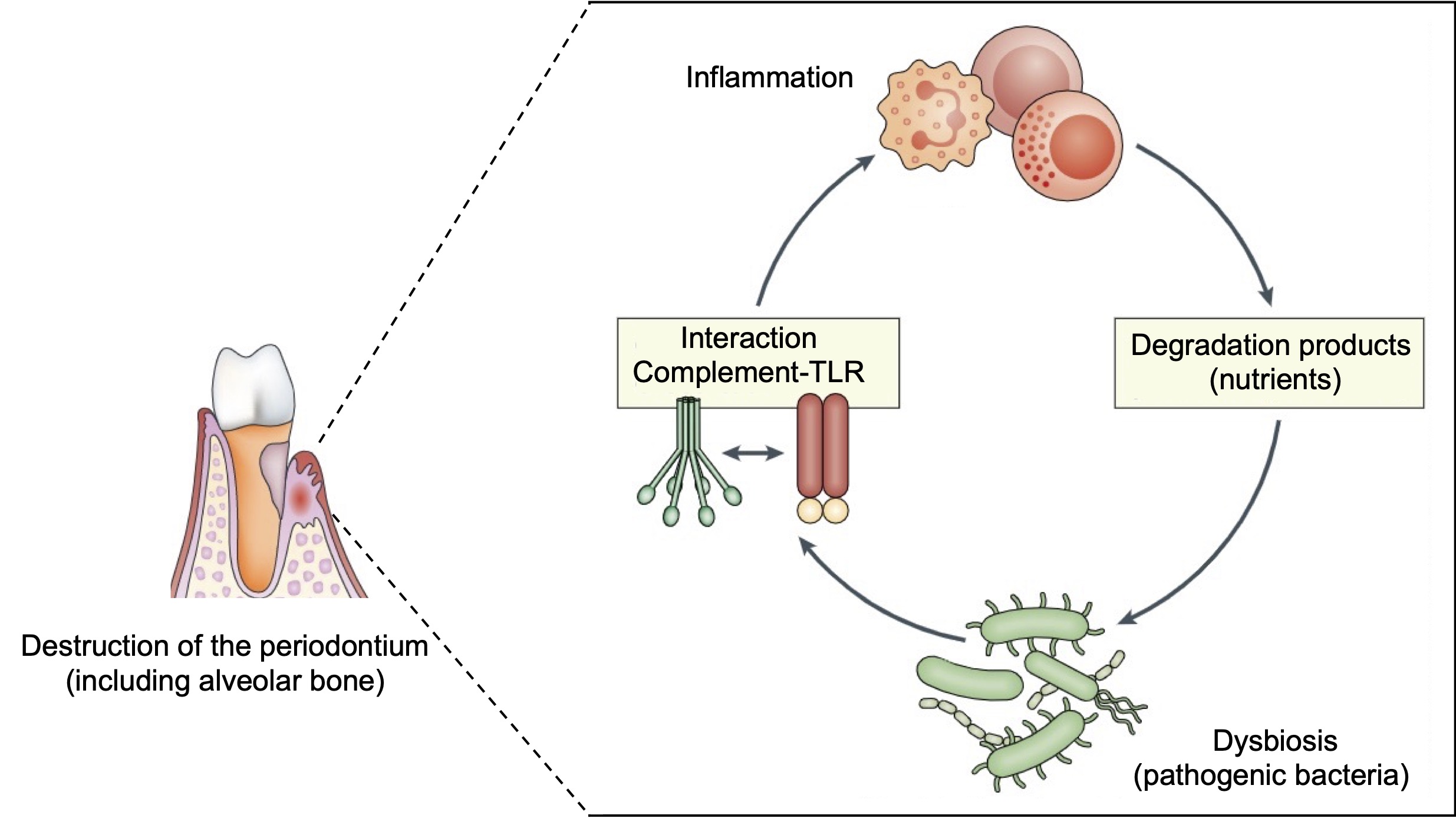
Figure 3. Amplification of the inflammatory response is responsible for the development of periodontitis. The imbalance of the microbiome of dental plaque (dysbiosis) leads to the activation of the immune defences (mainly the complement system and the Toll-like receptors (TLR)) and the triggering of an inflammatory response. This inflammation causes the destruction of the tissues surrounding the tooth, including the alveolar bone, which generates several nutrients that support the proliferation of pathogenic bacteria, adapted to grow in these inflammatory conditions. An amplification loop is therefore created in which inflammation promotes bacterial growth and vice versa, which supports the progression of periodontitis.
The mechanisms involved in this “immunodestruction” are extraordinarily complex and will not be described in detail here, but let us only mention that the sustained presence of periodontal bacteria activates certain defence systems specialized in the rapid response to infections (Toll-like receptors and complement system) present on the surface of immune cells, which activates the production of inflammatory molecules that are very irritating to the surrounding tissues. In the alveolar bone, for example, the production of cytokines (interleukin-17, in particular) stimulates the cells involved in the breakdown of bone tissue (osteoclasts) and leads to bone resorption.
It is important to mention that even if the initiation of periodontitis depends on the presence of pathogenic bacteria in dental plaque, the evolution of the disease remains strongly influenced by several factors, both genetic and associated with lifestyle. For example, there is a strong genetic predisposition to periodontal disease, with an estimated heritability of 50%: some people do not develop periodontitis despite a massive build-up of tartar (and bacteria) around the teeth, while others will be affected by the disease despite a small amount of dental plaque. These differences in susceptibility to periodontitis are thought to be caused by the presence of variations (polymorphisms) in certain genes involved in the inflammatory response.
In terms of lifestyle habits, the nature of the diet, certain metabolic diseases such as obesity and type 2 diabetes, stress and smoking are well-documented aggravating factors for periodontitis. This influence is particularly dramatic for smoking, which has catastrophic effects on the onset, progression and severity of periodontitis, with an increase in the risk of the disease that can reach more than 25 times (see Table 3). It should be noted that a common point to all of these risk factors is that they all influence in one way or another the degree of inflammation, which highlights to what extent the development of periodontitis depends on the intensity of the host’s inflammatory response in reaction to the presence of pathogenic bacteria in dental plaque.
Periodontitis and cardiovascular disease
Although the damage caused by this disproportionate inflammatory response is first and foremost local, at the level of the tissues surrounding the tooth, the fact remains that the inflammatory molecules that are generated at the site of infection are in close contact with the bloodstream and can therefore diffuse into the blood and affect the whole body. The impact of this systemic inflammation is probably very important, as numerous studies have reported that the incidence of periodontitis is strongly correlated with the presence of several other diseases (comorbidities) whose development is influenced by chronic inflammation, in particular cardiovascular disease, diabetes, certain cancers and arthritis (Table 1).
Table 1. Association of periodontitis with different pathologies.
Comorbidities of periodontitis Observed phenomena Sources
Cardiovascular disease Periodontitis is associated with an increased risk of heart attack and stroke. See Table 2 references.
Diabetes (types 1 and 2) Chronic inflammation associated with diabetes accelerates the destruction of periodontal tissues. Lalla and Papapanou (2011)
This association between the two diseases is bidirectional, as the chronic inflammation generated by periodontitis increases insulin resistance and in turn disrupts blood sugar control.
Alzheimer's Several epidemiological studies have reported an association between periodontitis and the risk of developing Alzheimer’s disease. Dioguardi et al. (2020)
The periodontal bacterium P. gingivalis (DNA, proteases) has been detected in the brains of patients who have died of Alzheimer’s disease as well as in the cerebrospinal fluid of people suffering from the disease. Dominy et al. (2019)
The risk of mortality from Alzheimer’s disease is correlated with antibody levels to a group of periodontal bacteria, including P. gingivalis, Campylobacter rectus, and Prevotella melaninogenica. Beydoun et al. (2020)
Rheumatoid arthritis Several epidemiological studies have observed an association between periodontitis and rheumatoid arthritis. Sher et al. (2014)
The inflammation caused by periodontitis stimulates the production of cells that increase bone resorption in the joints. Zhao et al. (2020)
Cancer The incidence of colorectal cancer is 50% higher in individuals with a history of periodontitis. Janati et al. (2022)
A periodontal bacterium (Fusobacterium nucleatum) has been repeatedly observed in colorectal cancers. Castellarin et al. (2011)
High levels of P. gingivalis have been detected in oral cancers. Katz et al. (2011)
High levels of antibodies against P. gingivalis are associated with a 2-fold higher risk of pancreatic cancer. Michaud et al. (2013)
Liver diseases Periodontitis is correlated with an increased incidence of liver disease. Helenius-Hietala et al. (2019)
In patients with fatty liver disease or non-alcoholic steatohepatitis, treatment of periodontitis decreases blood levels of markers of liver damage. Yoneda et al. (2012)
Intestinal diseases Chronic inflammatory bowel disease is associated with an increased risk of periodontitis. Papageorgiou et al. (2017)
This relationship is bidirectional, as periodontal bacteria ingested via saliva contribute to intestinal inflammation and disrupt the microbiome and intestinal barrier. Kitamoto et al. (2020)
Pregnancy complications Maternal periodontitis is associated with a higher risk of undesirable pregnancy outcomes such as miscarriages, premature deliveries, and low birth weight. Madianos et al. (2013)
Periodontal bacteria (P. gingivalis, F. nucleatum) have been observed in the placenta and clinical studies have reported a link between the presence of these bacteria and pregnancy complications. Han and Wang (2013)
The link between periodontitis and cardiovascular disease has been particularly studied because it is clearly established that inflammation participates in all stages of the development of atherosclerosis, from the appearance of the first lesions caused by the infiltration of white blood cells which store cholesterol, until the formation of clots that block blood circulation and cause heart attack and stroke. These inflammatory conditions are usually a consequence of certain lifestyle factors (smoking, poor diet, stress, physical inactivity), but can also be created by acute infections (influenza and COVID-19, for example) or chronic infections (Chlamydia pneumoniae, Helicobacter pylori, human immunodeficiency virus). Since all of these infections increase the risk of cardiovascular disease, it is therefore possible that a similar phenomenon exists for the chronic inflammation that results from periodontitis.
The first clue to the existence of a link between periodontitis and the risk of cardiovascular disease comes from a study published in 1989, where it was observed that a group of patients who had suffered a myocardial infarction had poorer oral health (more cavities, gingivitis, periodontitis) than a control group. Since then, hundreds of studies examining the issue have confirmed this association and shown that the presence of oral health problems, periodontitis in particular, is very often correlated with an increased risk of heart attack and stroke (Table 2).
Table 2. Summary of the main studies reporting an association between periodontitis and the risk of heart attack and stroke.
Measured parameter Observed phenomenon Sources
Coronary artery disease Periodontitis is associated with an increased risk of heart attack (men < 50 years). DeStefano et al. (1993)
Poor oral health (caries, periodontitis) is associated with an increased risk of heart attack and sudden death in coronary patients. Mattila et al. (1995)
Tooth loss caused by periodontitis is associated with an increased risk of heart attack and sudden death. Joshipura et al. (1996)
Bone loss caused by periodontitis is associated with an increased risk of heart attack, fatal and non-fatal. Beck et al. (1996)
The severity of periodontitis (bone loss) is associated with an increased risk of heart attack. Arbes et al. (1999)
Periodontitis is associated with an increased risk of fatal infarction. Morrison et al. (1999)
Periodontitis is associated with a slight (non-significant) increase in the risk of coronary heart attacks. Hujoel et al. (2000)
Periodontitis is associated with a slight (non-significant) increase in the risk of heart attack. Howell et al. (2001)
Bleeding gums are correlated with a higher risk of heart attack. Buhlin et al. (2002)
Periodontitis is associated with a higher risk of hospitalization for heart attack, angina or unstable angina. López et al. (2002)
High levels of antibodies against two pathogens responsible for periodontitis (A. actinomycetemcomitans and P. gingivalis) are associated with an increased risk of coronary heart disease. Pussinen et al. (2003)
Coronary patients more often experience poor oral health and an increase in inflammatory markers. Meurman et al. (2003)
Periodontitis is associated with an increased risk of mortality from coronary heart disease. Ajwani et al. (2003)
High levels of antibodies against a bacterium responsible for periodontitis (P. gingivalis) are associated with an increased risk of heart attack. Pussinen et al. (2004)
Periodontitis is associated with an increase (15%) in the risk of coronary heart disease (meta-analysis). Khader et al. (2004)
Periodontitis, combined with tooth loss, is associated with an increased risk of coronary heart disease. Elter et al. (2004)
Oral pathologies are more common in coronary patients. Janket et al. (2004)
Periodontitis is more common in coronary patients. Geerts et al. (2004)
High levels of antibodies against the bacteria responsible for periodontitis are associated with an increased risk of coronary heart disease in both smokers and non-smokers. Beck et al. (2005)
Higher levels of antibodies to bacteria involved in periodontitis (P. gingivalis and A. actinomycetemcomitans) are associated with an increased risk of coronary heart disease. Pussinen et al. (2005)
The presence of deep periodontal pockets is more common in women with coronary artery disease. Buhlin et al. (2005)
Periodontitis is associated with a higher risk of acute infarction. Cueto et al. (2005)
Periodontitis and levels of pathogenic bacteria (A. actinomycetemcomitans in particular) in the subgingival biofilm are associated with an increased risk of coronary heart disease. Spahr et al. (2006)
Periodontitis is more common in patients with coronary artery disease. Geismar et al. (2006)
Poor periodontal health is associated with an increased risk of coronary heart disease. Briggs et al. (2006)
Gingivitis, cavities and tooth loss are all associated with an increased risk of angina. Ylostalo et al. (2006)
Patients with acute coronary syndrome are at greater risk of being affected by periodontitis simultaneously. Accarini and de Godoy (2006)
The severity of periodontitis (bone loss) is associated with an increased risk of heart attack in 40-60 year-olds. Holmlund et al. (2006)
Patients affected by periodontitis have an increased risk (15%) of coronary heart disease (meta-analysis). Bahekar et al. (2007)
Periodontitis is associated with an increased risk of acute coronary syndrome. Rech et al. (2007)
Patients with acute coronary syndrome are more likely to have oral microbial flora enriched with periodontitis-causing bacteria. Rubenfire et al. (2007)
Periodontitis is associated with an increased risk of heart attack in both men and women. Andriankaja et al. (2007)
Coronary patients have deeper periodontal pockets and higher levels of a bacterium (Prevotella intermidia) involved in periodontitis. Nonnenmacher et al. (2007)
Men and women with < 10 teeth have a higher risk of coronary heart disease than those with > 25 teeth. Hung et al. (2007)
The severity of coronary artery disease (number of vessels affected) is correlated with the severity of periodontal disease. Gotsman et al. (2007)
Severe periodontitis is more common in patients with coronary artery disease. Starkhammar Johansson et al. (2008)
Chronic periodontitis is associated with an increased risk of coronary heart disease in men < 60 years of age. Dietrich et al. (2008)
Periodontitis is associated with an increased risk of angina and heart attack in both men and women. Senba et al. (2008)
Higher levels of antibodies to bacteria involved in periodontitis (P. gingivalis, A. actinomycetemcomitans, T. forsythia, and T. denticola) are associated with an increased risk of heart attack. Lund Håheim et al. (2008)
Higher levels of antibodies to bacteria involved in periodontitis (P. gingivalis and A. actinomycetemcomitans) are associated with increased coronary artery calcification in type 1 diabetics. Colhoun et al. (2008)
The severity of periodontitis is correlated with greater blockage of the coronary arteries. Amabile et al. (2008)
The risk of coronary injury is higher (34%) in patients with periodontitis (meta-analysis). Blaizot et al. (2009)
Periodontitis is associated with a 24-35% increase in the risk of coronary heart disease (meta-analysis). Sanz et al. (2010)
Mortality from coronary heart disease is 7 times higher in patients with < 10 teeth compared to those with > 25 teeth. Holmlund et al. (2010)
High levels of two bacteria involved in periodontitis (Tannerella forsythensis and Prevotella intermedia) are correlated with an increased risk of heart attack. Andriankaja et al. (2011)
Periodontitis is associated with a higher risk of heart attack, regardless of smoking and diabetes. Rydén et al. (2016)
Periodontitis is associated with a twice as high risk of a heart attack (meta-analysis). Shi et al. (2016)
Patients with periodontitis are at higher risk of heart attack, cardiovascular mortality and all-cause mortality. Hansen et al. (2016)
Periodontitis doubles the risk of a heart attack (meta-analysis). Xu et al. (2017)
Oral infections in childhood (including cavities and periodontitis) are associated with the thickening of the carotid wall in adulthood. Pussinen et al. (2019)
Periodontitis and tooth loss are associated with a higher risk of coronary heart disease (meta-analysis). Gao et al. (2021)
Inflammation caused by periodontitis is associated with an increased risk of cardiovascular events. Van Dyke et al. (2021)
People affected by periodontitis have an increased risk of coronary heart attacks and premature mortality. Bengtsson et al. (2021)
Stroke Bone loss caused by periodontitis is associated with an increased risk of stroke. Beck et al. (1996)
Poor oral health is associated with an increased risk of stroke in men > 60 years of age. Loesche et al. (1998)
Severe gingivitis, periodontitis and tooth loss are associated with an increased risk of fatal stroke. Morrison et al. (1999)
Periodontitis is associated with an increased risk of stroke (non-hemorrhagic). Wu et al. (2000)
Periodontitis is associated with a slight (non-significant) increase in the risk of stroke. Howell et al. (2001)
Bleeding gums are associated with a higher risk of stroke. Buhlin et al. (2002)
Periodontitis and tooth loss (< 24 teeth) are associated with an increased risk of stroke. Joshipura et al. (2003)
The risk of stroke associated with periodontitis is 2 times higher than the risk of coronary heart disease (2.85 vs 1.44) Janket et al. (2003)
Severe periodontitis (bone loss) is associated with an increased risk of stroke. Elter et al. (2003)
Severe periodontitis is associated with an increased risk of stroke. Dorfer et al. (2004)
High levels of antibodies against two pathogens responsible for periodontitis (A. actinomycetemcomitans and P. gingivalis) are associated with an increased risk of stroke (primary and secondary). Pussinen et al. (2004)
Periodontitis is associated with an increased risk of stroke in men < 60 years of age. Grau et al. (2004)
Higher-than-normal tooth loss is associated with a higher risk of stroke-related mortality and all-cause mortality. Abnet et al. (2005)
Poor periodontal health is associated with an increased risk of stroke. Lee et al. (2006)
Higher levels of antibodies to a bacterium involved in periodontitis (P. gingivalis) are associated with an increased risk of stroke. Pussinen et al. (2007)
Loss of > 9 teeth is associated with an increased risk of stroke. Tu et al. (2007)
Periodontitis is associated with an increased risk of stroke in 60-year-old and normotensive men. Sim et al. (2008)
The loss of > 7 teeth is associated with an increased risk of stroke (ischemic and hemorrhagic). Choe et al. (2009)
Bone loss caused by periodontitis is associated with a higher risk of stroke, especially in men < 65 years of age. Jimenez et al. (2009)
The loss of > 17 teeth is associated with an increase in inflammatory markers and an increased risk of stroke. You et al. (2009)
Periodontitis is associated with an increased risk of fatal stroke. Holmlund et al. (2010)
Periodontitis (periodontal pocket > 4.5 mm) is associated with an increased risk of stroke. Pradeep et al. (2010)
Periodontitis is associated with an increased risk of hemorrhagic stroke in obese men. Kim et al. (2010)
Patients with periodontitis are at greater risk of stroke, cardiovascular mortality and all-cause mortality. Hansen et al. (2016)
Periodontitis is associated with an increased risk of carotid atherosclerosis (meta-analysis) Zeng et al. (2016)
The severity of periodontitis is associated with an increased risk of stroke. Conversely, regular dental care is associated with a decreased risk. Sen et al. (2018)
Periodontitis is associated with an increased risk of stroke affecting the major arteries. Mascari et al. (2021)
Bacterial invasion
In addition to the chronic inflammation generated by gum infection, it has also been proposed that damage to periodontal tissues may provide bacteria with an entry point into the circulation, a phenomenon similar to that frequently observed for many pathogen agents (about 50 bacterial species and many viruses). One of the best examples is arguably endocarditis, an infection that occurs when bacteria from dental plaque enter the bloodstream through the gums and attach themselves to the inner walls of the heart chambers and valves. It is for this reason that patients who need to undergo surgery to treat valvular heart conditions (the replacement or repair of heart valves) and who have dental problems are referred to their dentist to treat these conditions before the operation to prevent postoperative valve infection. In addition, patients with prosthetic heart valves or valvular pathologies are prescribed antibiotics before dental procedures to prevent endocarditis (bacterial infection of a heart valve).
Bacteremia (presence of bacteria in the blood) associated with periodontitis also allows pathogens to come into contact with the wall of blood vessels and penetrate the endothelial and muscle cells of these vessels, including at the level of atherosclerotic plaques. In this sense, it should be noted that infection with the main periodontal bacterium (P. gingivalis) is associated with an acceleration of the development of atherosclerosis in animal models, possibly in response to the innate inflammatory immune response directed against the bacterium at the vessel level. In sum, the link between periodontitis and cardiovascular disease is biologically plausible, whether due to the diffusion of inflammatory molecules that diffuse into the circulation or the presence of bacteria in the vessels.
Common risk factors
As a statement from the American Heart Association on the matter points out, however, it is difficult to demonstrate that these associations are causal, i.e., that periodontitis is directly responsible for the increased risk of CVD observed in these studies. This difficulty is largely due to the fact that the risk factors for periodontitis are very similar to those responsible for CV diseases (which are called in epidemiology confounding factors, i.e., variables that may influence both the risk factor and the disease being studied) (Table 3). The best example is undoubtedly smoking, which is both the most important risk factor for cardiovascular disease and periodontitis, but this similarity is also observed for all the “classic” cardiovascular risk factors, whether hypertension, diabetes, obesity, hypercholesterolemia or poor diet. In other words, what increases the risk of periodontitis also increases the risk of cardiovascular disease and vice versa, which makes it very difficult to establish a causal link between the two diseases.
Table 3. Similarity between risk factors for cardiovascular disease and periodontitis.
Cardiovascular risk factors Impact on the risk of periodontitis Sources
Smoking Compared to non-smokers, the risk of periodontitis is 18 times higher in smokers aged 20–49 and 25 times higher in smokers aged 50 and over. Hyman and Reid (2003)
Hypertension Periodontitis, especially severe forms of the disease, is associated with higher systolic and diastolic pressures and an increased risk of hypertension (≥140 mmHg systolic, ≥90 mmHg diastolic). Aguilera et al. (2020)
Dyslipidemias Periodontitis is associated with higher levels of LDL cholesterol and triglycerides, as well as lower levels of HDL cholesterol. Nepomuceno et al. (2017)
Diabetes (types 1 and 2) See Table 1
Obesity Obesity, especially at the abdominal level, is associated with a higher prevalence of periodontitis in young adults. Al-Zahrani et al. (2003)
Diet quality
Fruit and vegetable deficiency A diet rich in fruits and vegetables is associated with a decreased risk of periodontitis. Dodington et al. (2015)
Fibre and whole-grain deficiency High fibre intake is associated with lower prevalence and severity of periodontitis. Nielsen et al. (2016)
The protective effect of fibre contributes to the decrease in the risk of periodontitis associated with a high intake of whole grains. Merchant et al. (2006)
High intake of simple carbohydrates Consumption of added sugars is associated with an increase of about 50% in the prevalence of periodontitis (and caries). Lula et al. (2014)
High intake of saturated fats A greater portion of energy intake in the form of saturated fats is associated with an increased risk of periodontitis, possibly due to the pro-inflammatory action of these fatty acids. Iwasaki et al. (2011)
That being said, some studies have tried to establish this link by adjusting the risk of periodontitis to take into account the impact of these confounding factors. For example, the Swedish PAROKRANK study reported a significant increase (28%) in the risk of a first heart attack in people affected by periodontitis, even after subtracting the contribution of the main cardiovascular risk factors. According to the currently available clinical data, it is estimated that periodontitis could be an independent risk factor for cardiovascular disease, with an increase of about 10–15% in risk.
Beneficial treatment
A causal link between periodontitis and cardiovascular disease is also suggested by certain studies showing that periodontal treatments (scaling and root planing) are associated with an improvement in certain cardiovascular health parameters and/or a decrease in cardiovascular events. For example, in patients with periodontitis, removal of subgingival plaque by root planing (under local anesthesia) resulted in improved endothelial function (dilation of vessels by blood flow) within 6 months of treatment. Several other studies have confirmed this positive impact of periodontal treatment on vessel function as well as on other important parameters of cardiovascular health, such as levels of inflammatory molecules and cholesterol levels (total, LDL and HDL). This improvement is particularly noticeable in patients with comorbidities such as metabolic syndrome, diabetes or cardiovascular disease, suggesting that periodontal treatment may be useful for patients at high risk of cardiovascular events. In this sense, it is interesting to note that a recent study reported that periodontal treatment of patients with a recent stroke was associated with a decrease in the overall risk of cardiovascular events in the following year, as measured by a combination of the incidence of stroke, infarction and sudden death.
Overall, these studies raise the possibility that the development of cardiovascular disease may indeed be directly influenced by the presence of periodontal lesions. This close link illustrates how an imbalance affecting one part of the body, in this case the tissues surrounding the teeth, can negatively influence the entire human body. Good health is a global state: even if our organs each have a well-defined role, their proper functioning remains strongly influenced by the general conditions prevailing throughout the body. This is particularly true with regard to inflammation, a condition that favours the development of all chronic diseases and which is responsible for the majority of deaths affecting the population. In this context, the increased risk of several diseases associated with periodontitis, especially cardiovascular disease, is not so surprising, since it essentially represents another example of the damage that can be caused by the presence of these chronic inflammatory conditions.
The close association between oral and cardiovascular health therefore suggests that the prevention and treatment of periodontitis may play important roles in the prevention of cardiovascular disease, particularly in those at higher risk due to being overweight, diabetes or a history of cardiovascular disease. This important link between the teeth and the rest of the body unfortunately remains under-exploited because medicine and dentistry are distinct disciplines, which have evolved in parallel, without much interaction between them. While one can be treated for free for all diseases that affect the body (in Canada), dental care does not benefit from this coverage and is therefore out of reach for those less well off. There is no doubt that this situation contributes to the high prevalence of periodontitis in our society and to the negative repercussions associated with these infections on health in general. Extending health insurance to cover dental care would therefore be an important step forward for cardiovascular prevention and the prevention of several other chronic diseases.