Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesUpdated May 22, 2018
In animals, detecting a threat (smell of smoke, sight of a predator, sound of a gunshot) by the sensory organs (nose, eyes, ears) triggers a maximum alert in the brain that will initiate a series of extremely complex processes called the “fight-or-flight response.” By activating the adrenal glands, the brain controls the release of action hormones such as adrenaline into the blood in order to increase the respiratory rate, the heartbeat, the oxygen supply to the tissues, as well as the level of wakefulness and cerebral attention. All these changes are triggered so the animal can quickly fight or flee the danger. This is biological stress, essential to the survival of individuals and, consequently, of their species. Depending on the duration of the metabolic reactions, three categories of effects can be distinguished: 1) the immediate effects caused by the production of adrenaline and norepinephrine by the sympathetic nervous system (duration of a few seconds); 2) the intermediate effects from the secretion of adrenaline and norepinephrine by the medulla of the adrenal glands (duration of a few minutes); and 3) the prolonged effects caused by the hypothalamic-pituitary-adrenal (or corticotropic) axis, vasopressin and thyroxine (duration of a few hours, up to weeks).
Corticotropic axis
When a stressful situation occurs, neuronal signals are produced in the brain by the limbic system (amygdala, hippocampus) and transmitted to the hypothalamus (see Figure 1).
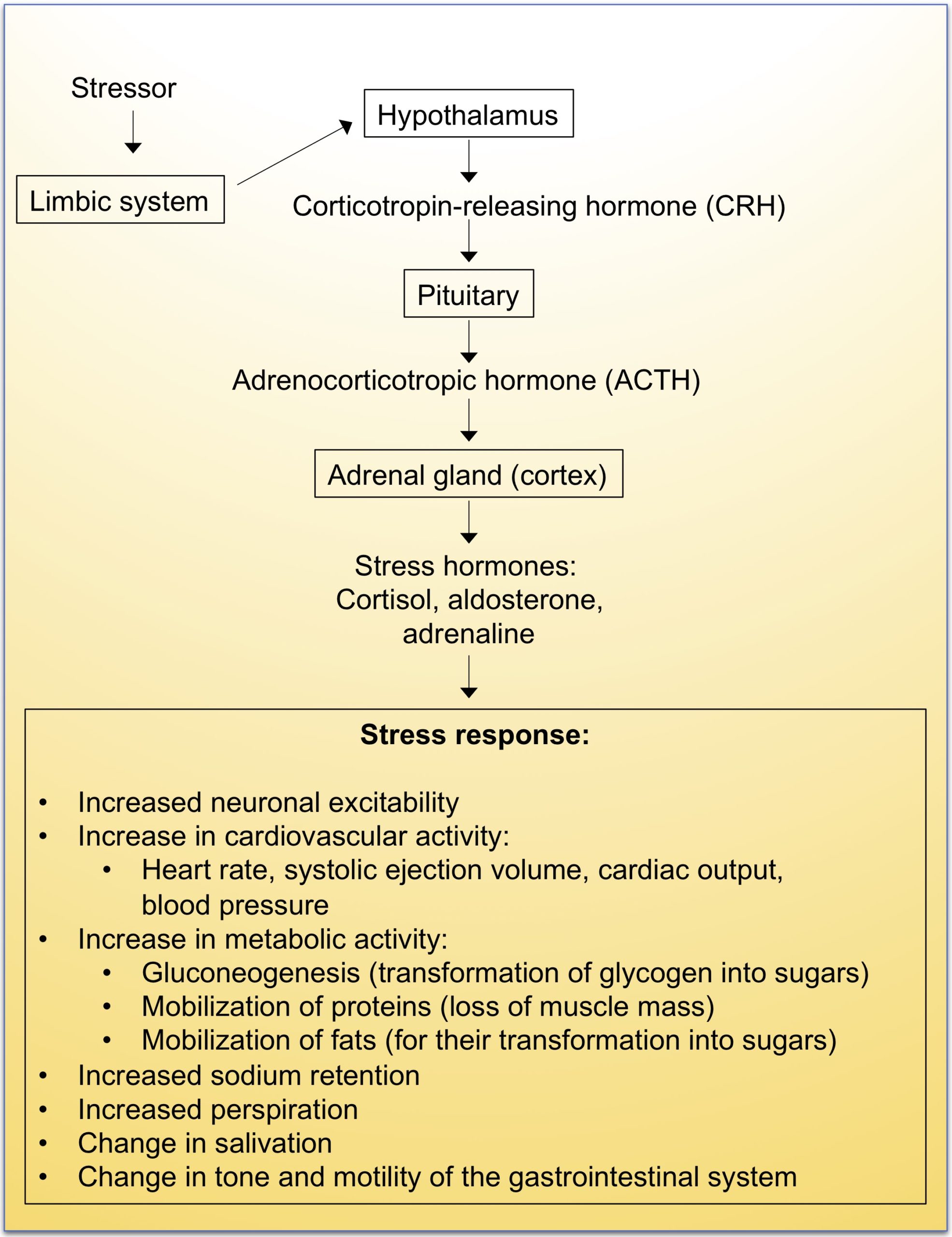
Figure 1. Corticotropic axis. Adapted from Managing stress:
Principles and Strategies for Health and Well-being, Fifth edition, 2005.
In response to this signal, the hypothalamus secretes the corticotropin-releasing hormone (CRH) that activates the pituitary gland, an endocrine gland that secretes several hormones including adrenocorticotropin (ACTH). This hormone is rapidly recognized by specific receptors present in the adrenal glands, which triggers the secretion of corticosteroids (cortisol, aldosterone) and adrenaline. The stress response is relayed by these messengers, which has the effect of increasing metabolism (more energy sources) and blood pressure. Cortisol increases blood pressure and blood sugar levels and inhibits the immune system. Catecholamines (adrenaline and norepinephrine) facilitate the fast and powerful use of muscles. Adrenaline binds to liver cell receptors and stimulates glucose production. Cortisol also induces the transformation of fatty acids into sugars and gluconeogenesis (glucose production from glycogen), which allows a significant energy supply to the muscles in order to escape or fight the stress-generating situation.
Effects of intense stress on the heart
Intense stress has a very important effect on the sympathetic autonomic nervous system that, along with hormones such as adrenaline, directly stimulates the heart. These changes accelerate the heart rate, cause severe cardiac arrhythmias, and may cause coronary arteries to contract. A good example of the negative impact of stress is the dramatic rise in sudden death that follows a tragic event: in the weeks following the earthquake off Sendai and the powerful tsunami that devastated this northeastern region of Japan in 2011, the number of people who died suddenly doubled compared to previous years, a trend that was maintained within three weeks of the initial shock (Figure 2). An increase in sudden mortality has also been observed following other major earthquakes (see here and here), illustrating how the physiological response to acute stress can have a negative impact on the heart.

Figure 2. Increased number of cardiac arrests during the Great East Japan Earthquake in 2011, in the three most affected prefectures (Iwate, Miyagi, Fukushima). Source: Kitamura et al. (2013).
Broken heart syndrome or takotsubo cardiomyopathy
People who do not have coronary heart disease but who are subjected to intense emotional stress may suffer from syndromes known by various names: broken heart syndrome, takotsubo cardiomyopathy, transient left ventricular apical ballooning syndrome, myocardial stunning, and neurogenic stress cardiomyopathy. These syndromes, which have common pathophysiological characteristics, are grouped together under the term “stress-induced cardiomyopathies.” Stress-induced cardiomyopathies without neurological impairment mainly affect women (80–90% of patients), especially postmenopausal women. In most cases, emotional or physical stress occurred before the onset of symptoms. Originally described in 1990 by Japanese cardiologists, takotsubo syndrome occurs when a person is exposed to significant stress or very bad news and suddenly develops high-intensity chest pain, secondary to myocardial infarction. If the person survives (which is usually the case), acute myocardial infarction is noted on arrival at the hospital, but without any arterial injury, i.e., without any blockage of the coronary artery. The name takotsubo comes from the shape of the left ventricle during the angiography exam (Figure 3), which is shaped like a vase (壺, tsubo) that resembles a trap that Japanese fishermen use to catch octopuses (蛸, tako). This phenomenon is caused by severe damage to the left ventricle, which is the region of the heart muscle that pumps arterial blood to the body. Several triggers have been identified over the years, most of them associated with strong negative emotions such as grief, anger or fear. Recent results, however, indicate that strong positive emotions (marriage, victory of a sports team) can also cause the onset of this syndrome.
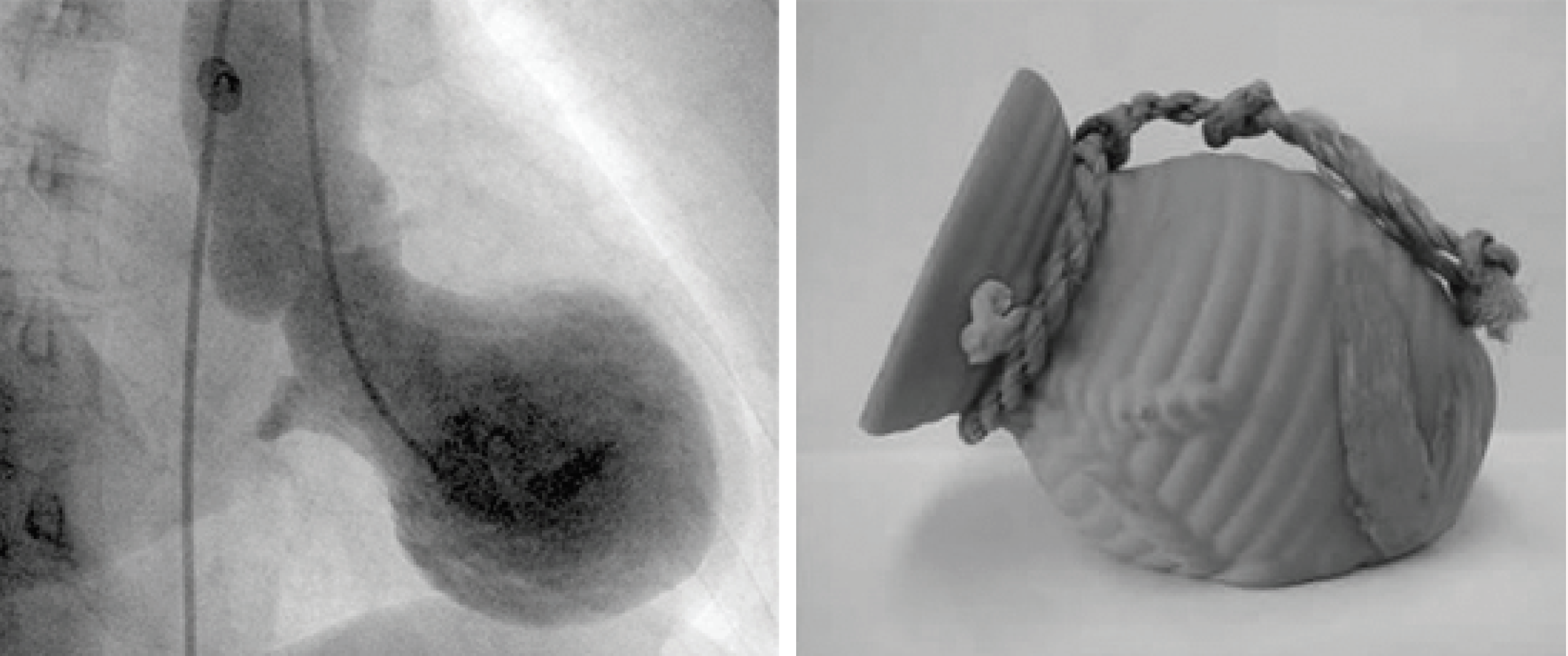
Figure 3. Left illustration: Angiographic imaging of a heart of a person suffering from a takotsubo.
Right image: The octopus trap (takotsubo) used by fishermen in Japan.
Chronic stress
Aside from these rather extraordinary examples that demonstrate the dramatic effects that the brain and our emotions may have on the heart, thousands of studies have been published on the effect of chronic stress, negative emotions, anxiety, depression, anger and hostility on the incidence of long-term coronary heart disease. In the 1940s and 1950s, early psychosomaticists, namely psychiatrists (usually psychoanalysts), became interested in the psychological characteristics that appeared to be associated with patients with coronary artery disease. Subsequently, in the 1960s, two cardiologists, R. H. Rosenman and Meyer Friedman, described the Type A personality, referring to people who are always in a hurry, are impatient, and have difficulty managing their aggressiveness. Having this type of personality seemed linked to the onset of coronary heart disease, but this link is still quite controversial today. Research on the subject suggests that it is rather two components present in Type A personalities, anger and hostility, that constitute important risk factors. Indeed, a meta-analysis of 25 studies has shown that both of these emotions are associated with a higher risk of having a myocardial infarction. They are also linked to a greater risk of recurrence according to 19 studies in patients who have already suffered a cardiac event.
Despite extensive evidence of a strong link between the brain and cardiovascular disease, this issue has been relatively under the radar of cardiologists until the publication of the Canadian cardiologist Salim Yusuf’s INTERHEART study. This major study, conducted among more than 24,000 people in 52 different countries, aimed to determine the main risk factors for myocardial infarction. Originally, Dr. Yusuf’s primary focus was on the classic risk factors of cholesterol, hypertension, abdominal obesity, and tobacco, but he decided to also observe measures of perceived or objective stress in the patients, even though he wasn’t convinced of its effects. A relevant addition, as the study demonstrated that “psychosocial” stress is indeed associated with an increased risk of myocardial infarction and that this effect, although less important than smoking, is comparable to the effect of hypertension and abdominal obesity. Dr. Yusuf concluded his article by emphasizing that psychosocial factors are far more important than previously recognized, and that they can contribute to a “substantial” proportion of myocardial infarction in all societies. Several mechanisms can explain the effect of stress on the cardiovascular system and, in particular, the coronary arteries: inflammation, increase in blood coagulability, decrease in fibrinolysis (ability of blood to dissolve clots), and increased circulating catecholamines (adrenaline and norepinephrine hormones), which, among other effects, accelerate the heart and increase its force of contraction (Figure 4).

Figure 4. The pathophysiological effects of acute psychosocial stress.
Source: Piña et al., J. Am. Coll. Cardiol. 2018.
Depression and cardiovascular disease
With respect to depression, several studies report that a depressive state after myocardial infarction increases the risk of death in the months following discharge from hospital. A study conducted at the Montreal Heart Institute by Dr. François Lespérance and his collaborators has shown that the presence of depression in hospitalized patients after an unstable angina episode increases the risk of fatal recurrence or infarction by 6 the year following hospital discharge.
Although stress and depression are now recognized as major risk factors for cardiovascular disease, studies on the treatment for these conditions using antidepressant or anxiolytic medications have not produced convincing results. This is a significant problem as up to 30–40% of patients experience depressive symptoms after myocardial infarction, which can greatly increase the risk of recurrence and premature death if not adequately treated. There is also a high rate of depression after cardiac surgery. At the Montreal Heart Institute’s EPIC Centre, for the past 30 years we have observed that a cardiac rehabilitation program that includes exercise training practiced two to three times a week at the Centre, alongside a group of patients with similar conditions, considerably improves depressive feelings and reduces stress after a cardiac event or surgery. When patients are asked what is most important to them after myocardial infarction, many of them say they would like to “reduce their stress.” Patients are also often convinced that the stress they are experiencing is the primary cause of their heart condition.
To successfully prevent recurrence, everything must therefore begin with the brain, because when stress and depressive states are well “managed” and priorities have been redefined, patients are prepared to significantly change their lifestyle habits. Unfortunately, patients from a low socioeconomic background have problems that medicine alone cannot remedy; they benefit the least from prevention programs, for many economic and social reasons. This situation is well documented in western countries. Indeed, poverty remains the biggest risk factor for premature death.
Stress management
How can you change your lifestyle habits when your psychological state is unstable? Based on my experience, the patients with the best outcomes are those who succeed in making quite drastic changes, either by themselves, because the heart attack or cardiac surgery has triggered a reassessment of their personal situation, or with the help of a multidisciplinary team and a stress management program.
Managing your stress — A few references
At the MHI’s EPIC Centre, workshops on stress management through mindfulness are led by Dr. Robert Béliveau and other professionals experienced in this approach. I encourage readers to look into this subject, especially by consulting the following books:
—Christophe André, Looking at Mindfulness;
—Matthieu Ricard, The Art of Meditation;
—Jon Kabat-Zinn, Full Catastrophe Living;
—Rick Hanson, Hardwiring Happiness.
For about ten years, we have been using the approach developed by Jon Kabat-Zinn of the Center for Mindfulness in the Faculty of Medicine at the University of Massachusetts in Boston, an approach called “mindfulness-based stress reduction.” This is a fairly intensive approach presented in eight two-and-a-half-hour-long weekly workshops. This method has proven its value for over 25 years, and many scientific articles have demonstrated its effectiveness, not only for reducing stress and improving overall quality of life but also for preventing recurrence after a cardiac event. For example, a study published in 2012 by R. H. Schneider and his colleagues confirms that practicing meditation for 20 minutes twice a day cuts relapses after a cardiac event in half in the five years following. By managing their stress much better, patients more easily adopt all the changes needed to avoid recurrence.
Should this approach also be used in primary prevention, before becoming ill? The answer is yes, absolutely. People with many risk factors or who have a mediocre quality of life owing to chronic stress can benefit greatly from the mindfulness-based approach.
What the neurosciences have taught us, and what Rick Hanson describes very well in his book Hardwiring Happiness (2013), is that the human brain first went through a “reptilian” stage during evolution, originally reinforcing our reactions to danger to give us a chance at survival. Obviously, the brain evolved and became much more complex with the development of the cerebral cortex, but traces of our reptilian brain are still there. We therefore have a tendency to view negative events as being three to five times more important than positive ones (see here and here). For example, Daniel Kahneman, who received the Nobel Prize in Economics in 2002 for his studies on this subject, observed that, given an equal amount of money, a financial loss is much more strongly felt than a gain. In other words, if you lose $1,000 on the stock market, the psychological impact will be as powerful as if you had won $5,000. The same holds true for our interpersonal relationships: a negative remark or behaviour directed at us has three to five times more impact than its positive equivalent. This tendency to overemphasize the negative has enabled humans to survive and evolve. For example, worrying and then making sure that there are no snakes hidden in a bush is a situation where the vigilance associated with worry results in avoiding a bite, whereas unconcern in the face of danger can cause death. Our brain is thus programmed to worry. To manage our stress well and improve our quality of life, we have to work actively at “reprogramming” it, so it gives more weight to the effects of positive experiences rather than of negative ones.
The approach suggested by Jon Kabat-Zinn, Christophe André, and Matthieu Ricard teaches us to take a moment to pause, carefully observe our physical and psychological reactions, and modify our perceptions and behaviours. Contrary to what many people think, meditation is not a relaxation technique, nor a way to hide our problems. Quite the opposite: the goal is to pause briefly, concentrate on the present moment, and observe our thoughts so as to transform the way we think. It is not a means of relaxation, but rather a means of transformation.