Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesOver the past few years, we have repeatedly commented (here, here, and here) on the research that has looked at the benefits associated with intermittent fasting and calorie restriction in general. In this article, we approach this subject from a more general angle: how can we explain that the simple fact of restricting caloric intake to a shorter window of time can lead to such benefits?
It is now clearly established that what we eat daily has a huge influence on the development of all chronic diseases. As we have mentioned several times, many studies have indeed shown that a high intake of plants (fruits, vegetables, whole grains, legumes, nuts and seeds) is associated with a significant reduction in the risk of these diseases, while conversely, the risk of overweight, cardiovascular disease, type 2 diabetes, several types of cancer and premature mortality is increased by excessive consumption of animal products (meat and deli meats in particular) as well as ultra-processed industrial foods.
However, diet quality does not seem to be the only parameter that can modulate the risk of these chronic diseases; indeed, many studies carried out in recent years suggest that the period of time during which food is consumed also plays a very important role. For example, preclinical studies have revealed that rodents that have continuous access to food rich in sugar and fat develop excess weight and several metabolic disturbances implicated in the genesis of chronic diseases (insulin resistance, in particular), while those who eat the same amount of food, but in a shorter amount of time, do not show these metabolic abnormalities and do not accumulate excess weight.
In other words, it would not only be the amount of calories that matters, but also the window of time during which these calories are consumed. This new concept of time-restricted eating (TRE) is truly revolutionary and is currently attracting enormous interest from the scientific and medical communities.
Intermittent fasting
Strictly speaking, time-restricted eating is a form of intermittent fasting since calorie intake is restricted to relatively short periods of the day (e.g., 6–8 h), alternating with periods of fasting ranging from 16 to 18 h (a popular formula is the 16:8 diet, i.e. a 16 h fast followed by an 8 h eating window). This type of intermittent fasting is generally easier to adopt than other more restrictive types of fasting such as the 5:2 diet, in which 5 days of normal eating is interspersed with 2 days (consecutive or not) where the calorie intake is zero or very low, or alternate day fasting (one day out of two of fasting, alternating). Since TRE is simply eating an early dinner or a late lunch to achieve a 16–18 h period of not eating, this type of intermittent fasting usually does not cause major lifestyle changes and is therefore within reach of most people.
Eating too much and too often
The interest in TRE and other forms of intermittent fasting can be seen, to some extent, as a reaction to the sharp increase in the number of overweight people observed in recent decades. Statistics show that 2/3 of Canadians are currently overweight (BMI>25), including a third who are obese (BMI>30), and this overweight has become so much the norm that we forget how much our collective waist circumference has skyrocketed over the past 50 years.
For example, statistics published by the US Centers for Disease Control and Prevention (CDC) indicate that between 1960 and 2010, the average weight of an American man increased from 166 pounds to 196 pounds (75 to 89 kg), while that of women increased from 140 pounds to 166 pounds (63 to 75 kg) (Figure 1). In other words, on average, a woman currently weighs the same as a man who lived during the ’60s! No wonder people are much thinner than they are today in family photos or movies from that era.
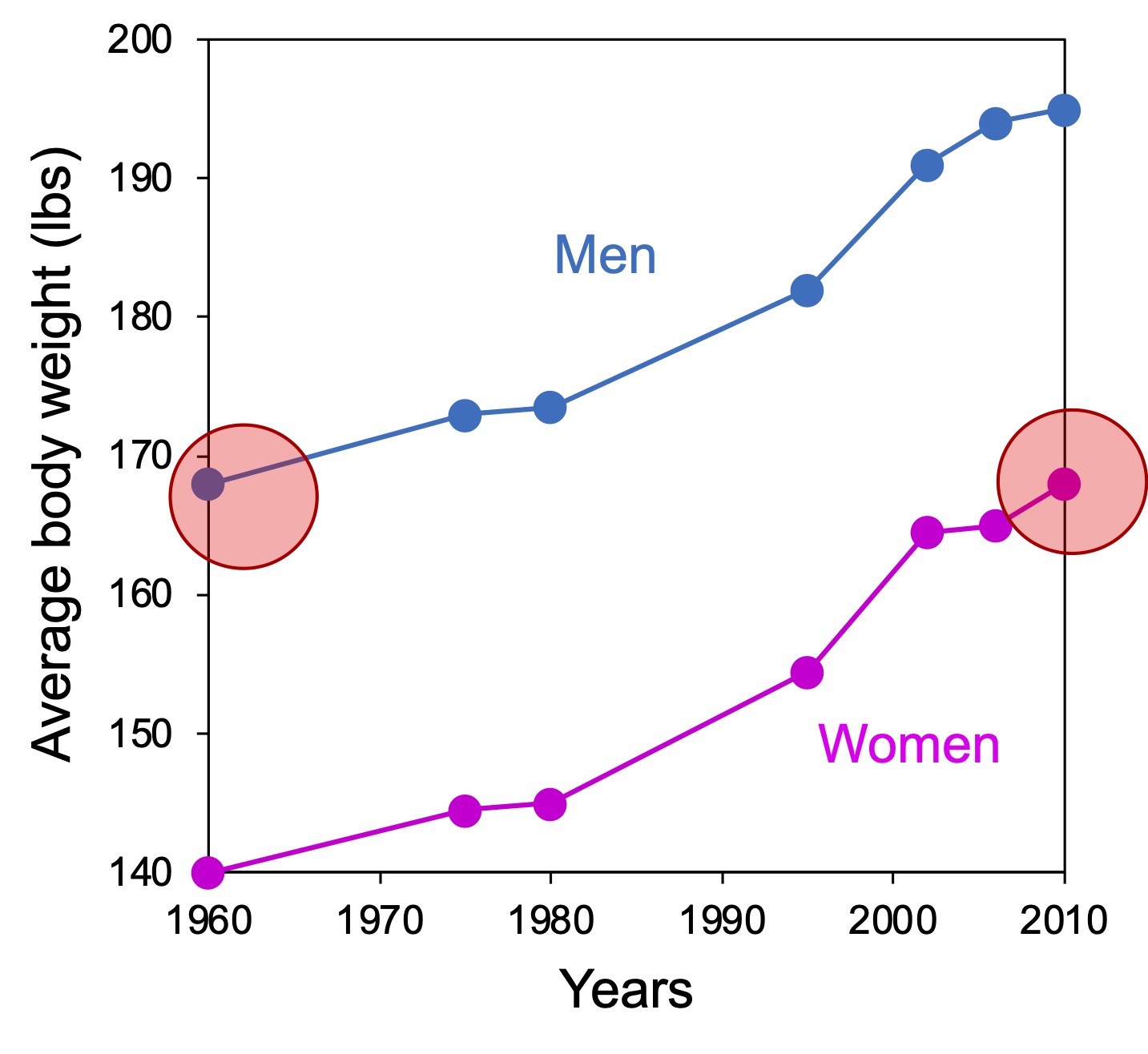
Figure 1. Increase in average body weight of the US population over the past decades. Adapted from data from the CDC. Note that the average weight of women in 2010 was identical to that of men in 1960 (red circles). A similar trend, as measured by the increase in the body mass index, has been observed in several regions of the world, including Quebec.
The overconsumption of calories, especially those from ultra-processed industrial foods, is certainly one of the main factors that have contributed to this rapid increase in the body weight of the population. The environment in which we live strongly encourages this excessive intake of energy (aggressive advertising, processed foods overloaded with sugar and fat, almost unlimited availability of food products), so that collectively we eat not only too much, but also too often. For example, a study carried out in the United States showed that what is generally considered to be the standard diet, i.e. the consumption of three meals a day spread over a period of 12 hours, is on the contrary a fairly marginal phenomenon (less than 10% of the population). In fact, the study showed that most people eat multiple times throughout the day (and evening), with an average interval of only 3 hours between calorie consumption periods. According to this study, more than half of the population consumes its food over a period of 15 hours or more per day, which obviously increases the risks of excessive energy intake. It should also be noted that these researchers observed that for the vast majority of participants, all the food consumed after 6:30 p.m. exceeded their energy needs.
Weight (and metabolism) control
Several studies suggest that intermittent fasting, including TRE, represents a valid approach to correct these excesses and restore the caloric balance essential for maintaining a normal body weight. Obviously, this is particularly true for obese people who eat more than 15 hours a day. For these people, simply reducing their eating window to 10–12 hours, without necessarily making special efforts to restrict their calorie intake, is associated with a reduction in body weight.
Most studies that have looked at the effect of TRE on body weight find similar results, namely that in overweight people, simply restricting the eating period to a window of 8–10 h generally leads to weight loss in the following weeks (Table 1). This loss is quite modest overall (2–4% of body weight), but can, however, become more significant when TRE is combined with a low-calorie diet.
It would, however, be reductionist to see TRE simply as an approach for controlling body weight. In practice, studies indicate that even in the absence of weight loss (or when the loss is very modest), TRE improves certain key aspects of metabolism. For example, in overweight, prediabetic men, reducing the eating window from 12 to 6 h for 5 weeks did not result in significant weight loss, but was nonetheless associated with lower resistance to insulin and fasting blood glucose. These results were confirmed by a subsequent study; in the latter case, however, the TRE-induced decrease in blood sugar only seems to occur when the eating window is in the first portion of the day (8 a.m.-5 p.m.) and is not observed for longer late windows (12 p.m.-9 p.m.). This superiority of TRE performed at the start of the day in reducing fasting blood glucose has been observed in other studies, but remains unexplained to date.
It should also be noted that these positive impacts of TRE on glucose metabolism are also observed in people of normal weight (BMI=22), which underlines how the benefits of TRE go far beyond simple weight loss.
Table 1. Examples of studies investigating the effects of TRE on body weight and metabolism.
| Eating window | Duration of the study | Participants | Key results | Source |
|---|---|---|---|---|
| 13 h (6 a.m.-7 p.m.) | 2 weeks | 29 M (avg. 21 years) BMI=25 | ↓ weight (-0.4 kg) ↓ caloric intake | LeCheminant et al. (2013) |
| 10–12 h (time at the choice of the participant) | 16 weeks | 5 M, 8 W (24–30 years) BMI>30 | ↓ weight (-3.3 kg) ↑ sleep quality | Gill and Panda (2015) |
| TRE: 8 h (1 p.m.-9 p.m.) Ctl: 13 h (8 a.m.-9 p.m.) | 8 weeks | 34 M BMI=30 | ←→ weight ↓IGF-1 ↓body fat | Moro et al. (2016) |
| TRE: 6 h (8 a.m.-2 p.m.) Ctl: 12 h (8 a.m.-8 p.m.) | 5 weeks | 8 M (avg. 56 years) BMI>25 and prediabetes | ←→ weight ↓insulin resistance ↓postprandial insulin ↓blood pressure ↓appetite in the evening | Sutton et al. (2018) |
| 8 h (10 a.m.-6 p.m.) | 12 weeks | 41 W, 5 M (avg. 50 years) BMI=35 | ↓ weight (-2.6%) ↓ caloric intake ↓ blood pressure | Gabel et al. (2018) |
| 3 h less than usual (breakfast 1.5 hours later; dinner 1.5 hours earlier) | 10 weeks | 12 W, 1 M (29–57 years) BMI=20-39 | ←→ weight ↓caloric intake ↓body fat | Antoni et al. (2018) |
| 9 h Early: 8 a.m.-5 p.m. Late: 12 p.m.-9 p.m. | 1 week | 15 M (avg. 55 years) BMI>25 | ↓ weight (-0.8 kg) ↓ postprandial blood glucose ↓ TG ↓ fasting blood glucose (only for early TRE) | Hutchison et al. (2019) |
| TRE: 8 h (12 p.m.-8 p.m.) Ctl: 3 meals at fixed times | 12 weeks | 70 M, 46 W (avg. 47 years) BMI>25 | ↓ weight (1.2%) for TRE (not significant) | Lowe et al. (2020) |
| 10 h (time of the participant’s choice) | 12 weeks | 13 M, 6 W (avg. 59 years) (with metabolic syndrome) | ↓weight ↓waist circumference ↓blood pressure ↓LDL cholesterol ↓HbA1C | Wilkinson et al. (2020) |
| 4 h (3 p.m.-7 p.m.) 6 h (1 p.m.-7 p.m.) | 8 weeks | 53 W, 5 M BMI>30 | ↓weight (3%) ↓insulin resistance ↓oxidative stress ↓caloric intake (-500 kCal/d on average) (no diff. between 4 h and 6 h) | Cienfuegos et al. (2020) |
| TRE: 10 h Ctl: 12 h (calorie deficit of 1000 kCal/d in both cases) | 8 weeks | 53 W, 7 M BMI>35 | higher weight loss for TRE vs. ctl (-8.5% vs. -7.1%) ↓ fasting blood glucose (only for TRE) | Peeke et al. (2021) |
| 8 h (12 p.m.-8 p.m.) | 12 weeks | 32 W BMI>32 | ↓weight (-4 kg) ↓CV risk (Framingham score) | Schroder et al. (2021) |
| 8 h (time of the participant’s choice) | 12 weeks | 37 W, 13 M BMI=35 | ↓weight (-5%) | Przulj et al. (2021) |
| TRE: 8 h (8 a.m.-4 p.m.) Ctl: 10 h (In both cases, calorie reduction to 1800 kCal/d for men and 1500 kCal/d for women) | 52 weeks | 71 M, 68 W (avg. 30 years) BMI>30 | higher weight loss for TRE vs. ctl (-8 kg vs. -6.3 kg) | Liu et al. (2022) |
| TRE: 8 h Early: 6 a.m.-2 p.m. Late: 11 a.m.-7 p.m. | 5 weeks | 64 W, 18 M BMI=22 | ↓caloric intake ↓insulin resistance (early TRE) ↓fasting blood glucose (early TRE) | Xie et al. (2022) |
| TRE: 10 h (from breakfast) Ctl: no time limit (calorie reduction of 35% in both cases) | 12 weeks | 69 W, 12 M (avg. 38 years) BMI=34 | higher weight loss for TRE vs. ctl (-6.2 kg vs. -5.1 kg) | Thomas et al. (2022) |
| ART: 8h (7h-15h) Ctl : ≥12h TRE: 8 h (7 a.m.-3 p.m.) Ctl: ≥12 h (calorie reduction of 500kCal/d in both cases) | 14 weeks | 72 W, 18 M (avg. 43 years) BMI>30 | higher weight loss for TRE vs. ctl (-6.3 kg vs. -4.0 kg) | Jamshed et al. (2022) |
Metabolic rhythms
The reasons for the positive impact of time-restricted eating are both very simple and eminently complex. First of all, simple in that we can intuitively understand that metabolism, like any job, requires periods of rest to optimize performance and avoid overheating and exhaustion.
During evolution, these metabolic work-rest cycles have developed in response to the Earth’s day-night cycle, which roughly corresponds to our sleep-wake cycle (Figure 2). During the day, we are in active mode and the main function of metabolism is to extract the energy contained in food (glucose, fatty acids, proteins) to meet the needs of the day. On the other hand, the metabolism is also predictable and economical, and a portion of this energy is not used immediately, but is rather stored in the form of glucose polymers (glycogen) or transformed into fat and stored at the level of adipose tissue to be used during more or less prolonged periods of fasting.
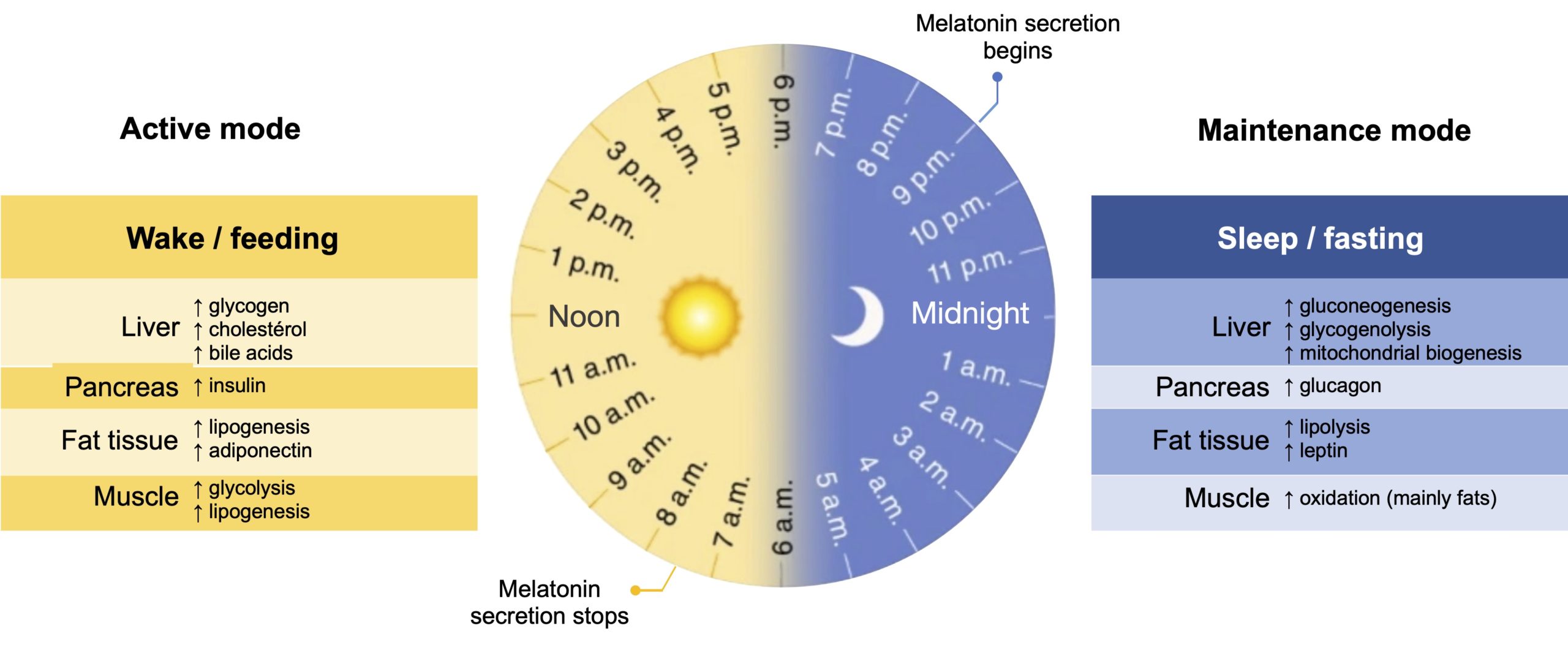
Figure 2. Rhythm of metabolic processes according to time of day. Most organisms, including humans, have evolved to have circadian rhythms (close to 24 hours) that create optimal time windows for rest, activity, and nutrient intake. This molecular clock coordinates appropriate metabolic responses with the light/dark cycle and improves energy efficiency through the temporal separation of anabolic (insulin secretion, glycogen synthesis, lipogenesis) and catabolic (lipolysis, glycogen breakdown) reactions in peripheral tissues. Disruptions in this cycle, for example following nutritional intake outside of the preferred time window, compromise organ functions and increase the risk of chronic disease. Adapted from Sassi and Sassone-Corsi (2018).
In this maintenance mode, which generally corresponds to the rest period (evening, night and beginning of the day), the function of the metabolism is to ensure that the energy supply to our cells remains adequate, even in the absence of food. Glucose stored as glycogen is first used to maintain blood sugar at a constant level, followed by a gradual transition in metabolism to the use of fat as the primary energy source. When the fasting period is prolonged, blood glucose levels become insufficient to keep the brain functioning (neurons are not able to use fatty acids as an energy source) and part of the fat is then used to produce ketone bodies. These ketone bodies can be metabolized by nerve cells (as well as cells in other organs, including muscles and the heart), allowing the body to not only survive a food deficiency, but also maintain physical and mental health needed to obtain this food (people who fast for longer periods of time (≥ 24 h) frequently report a noticeable improvement in their mental acuity). From an evolutionary perspective, this segmentation of metabolism into two distinct phases therefore developed to maximize energy extraction when food is available, while ensuring survival when it is not, during frequent periods of scarcity.
At the molecular level, this metabolic shift from glucose to fat therefore creates the equivalent of “work shifts” where the various enzymes and metabolic hormones active during the day are at rest during the night, while conversely, those which come into action during the night become inactive during the day.
One of the best examples of this finely orchestrated molecular choreography is the cycle governing the production of insulin. During the day, the cessation of melatonin secretion after waking allows the pancreas to produce insulin in response to carbohydrate ingestion, and the ensuing uptake of glucose from the bloodstream is used by cells to keep them functioning. At the same time, insulin also promotes the transformation of glucose into fatty acids in adipose tissue and the creation of an energy reserve for future use. In the evening, therefore at the start of the metabolic maintenance period, the secretion of melatonin (to promote sleep) interferes with that of insulin and the subsequent decrease in the entry of sugar into the cells facilitates the transition to the use of fat as the main source of energy during the rest period.
One of the immediate consequences of eating repeatedly over a long period of time during the day, for example 15 h or more as in the study mentioned earlier, is therefore to completely disrupt this insulin cycle. This is especially true for late evening calorie intake, when melatonin secretion normally signals the metabolism that energy extraction is complete for the day (insulin inhibition) and it is time to place oneself in the maintenance period. The ingestion of calories at this time then falls at a very bad moment, because both components of the metabolism are solicited at the same time and the ensuing cacophony simultaneously disrupts the normal functioning of each of them. For example, it has long been known that late caloric intake is associated with a higher increase in postprandial (post-meal) blood glucose.
Extended rest period
Limiting calorie intake to only 6–8 h of the waking period obviously has the immediate consequence of increasing the duration of the rest and maintenance period of the metabolism. It may not seem like much, but those few extra hours without caloric intake will force into motion a series of metabolic adaptations that are extremely important for the beneficial effects of TRE. This is where it gets complicated, but we can still try to simplify everything by separating these adaptations into two main categories:
- Optimizing the metabolic transition. As mentioned earlier, the fasting period is associated with the shift from a metabolism focused on glucose as the main source of energy towards fatty acids. On the other hand, when the fasting period is relatively short, around 12 h (for example, the end of dinner around 6 p.m. followed by breakfast at 6 a.m. the next day), this metabolic transition towards fat remains incomplete: the decrease in postprandial glucose levels is correlated with a slight increase in free fatty acids in circulation, but this increase is transient and cancelled upon ingestion of the first meal of the day (Figure 3, left graph). In addition, this time frame is not sufficient to generate significant levels of ketone bodies.
Figure 3. The impact of TRE on the metabolic transition to the use of fat as the main source of energy. After each meal, the blood glucose concentration rises rapidly within 15 minutes, peaking 30–60 minutes after the start of the meal, while the absorption of dietary triglycerides is much slower with a peak that occurs 3 to 5 hours later. This rapid rise in glucose results in a drastic increase in systemic insulin (~400–500 pmol/L) to allow glucose uptake and, simultaneously, acts on adipose tissue to inhibit the release of free fatty acids and block the production of ketone bodies. Therefore, the utilization of carbohydrates accounts for 70–75% of energy expenditure after the consumption of a meal. Hepatic glycogen metabolism then shifts from breakdown (glycogenolysis) to synthesis (glycogenesis) and muscle metabolism shifts from oxidation of fatty acids and amino acids to oxidation of glucose and storage of glycogen. This finely tuned response results in a decrease in blood glucose to <7.8 mmol/L two hours after a meal. During a standard fasting period (12 h) (left figure), blood glucose is maintained at a constant level (about 4.0-5.5 mmol/L), and it is the oxidation of fatty acids that becomes the main source of energy (about 45%, against 35% for glucose and 20% for proteins). When the fasting period exceeds 12 h (right figure), the concentration of glucose and insulin continues to slowly decrease, while that of free fatty acids increases to ensure the metabolic transition to fat oxidation. This transition is also associated with the production of ketone bodies in response to the influx of free fatty acids into the liver. Adapted from Dote-Monterro et al. (2022).
By postponing this first meal for a few hours (or by eating the last meal of the previous day earlier) in order to fast a little longer (16 h, for example), the absence of new food sources of sugar and triglycerides forces the metabolism to turn to the reserves of fatty acids as a source of energy as well as to begin the transformation of a part of these fats into ketone bodies to compensate for the scarcity of glucose (Figure 3, graph on the right).
In other words, by spreading caloric intake over an extended period of time (12+ hours), the excess energy stored as fat is almost never used. For people who regularly consume more calories than they need, there may therefore be a gradual accumulation of fat over time. On the other hand, by restricting this caloric intake over a shorter period of time (less than 12 h), the greater metabolic transition towards fats makes it possible to use these reserves and thus avoid the accumulation of a surplus of energy that can lead to overweight.
- Saving what you have gained. Another consequence of a prolonged period of fasting is to create a “climate of uncertainty” for the cells as to their future energy supply. If this shortage is prolonged, they then have no other choice but to adopt a cautious approach and to focus on maintaining their gains rather than considering continuing their expansion. To make a simple analogy, when times are tough, we devote our energies to maintaining the house and not to undertaking expansion work. This is exactly the approach favoured by the cells during a fast. In the absence of new sources of energy, the mechanisms involved in growth are put on hold and the residual energy is devoted instead to maintaining and repairing constituents essential to cellular integrity (DNA, mitochondria, proteins, etc.). This “rejuvenation cure” ensures that the general state of health of the cells is improved during a fast, which allows optimal functioning when the energy supply is restored.
Metabolic overheating
To better understand the impact of this adaptation to fasting on the metabolism, it may be useful to first visualize the extent to which the current standard diet, rich in foods of animal origin and ultra-processed foods (which alone currently account for nearly half of the daily calories consumed in Canada), is a perfect growth “cocktail” to create metabolic overheating and encourage the development of various pathologies.
This overheating is mainly caused by the simultaneous presence of two powerful activators of the signalling pathways involved in cell growth: free sugars and animal proteins (Figure 4). In particular, diets rich in protein and certain amino acids (methionine and branched-chain amino acids (BCAAs), mainly found in animal products) are the most effective in activating the GH/IGF-1 pathway involved in cell growth and premature aging. Under normal conditions, the activation of these growth pathways is obviously essential for survival, but when it becomes excessive, for example as a result of overconsumption of calories and/or too frequent food intake (for example over a period of 15 h, as observed in the study mentioned earlier), excess energy that is stored as fat can promote the development of resistance to the action of insulin (see our article on this subject). This insulin signalling disorder is truly problematic, as it catalyzes the onset of a series of metabolic upheavals that will create chronic inflammation and oxidative stress that are damaging to the entire body. These conditions can directly promote the development of the main chronic diseases (cardiovascular, type 2 diabetes, cancer, neurodegeneration) or even indirectly, by accelerating the aging process, one of the main risk factors for these diseases.
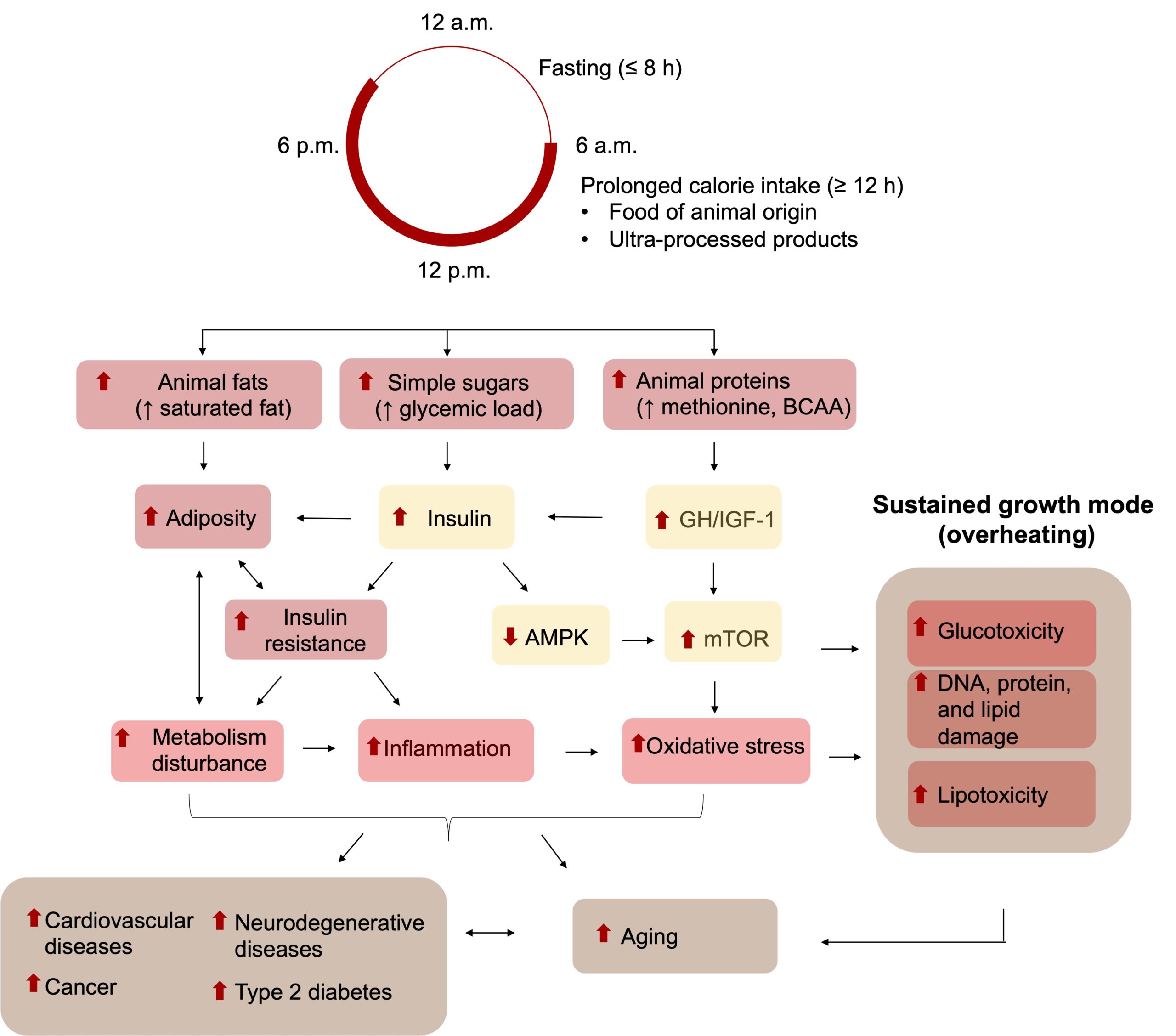
Figure 4. Effects of the standard Western diet on metabolism and the risk of chronic diseases. Prolonged daily caloric intake (≥12 h), combined with the presence of simple sugars and animal proteins, strongly activates the pathways involved in growth cells (GH/IGF-1, insulin) and promotes the development of metabolic abnormalities such as overweight and insulin resistance. The ensuing metabolic disturbances create a climate conducive to the development of conditions of chronic oxidative stress and inflammation that damage the cells (glucotoxicity, lipotoxicity, DNA damage, lipid damage and protein damage), accelerate biological aging, and increase the risk of several diseases.
Avoiding overheating
To simplify, we can see intermittent fasting, including TRE, as a way to minimize these risks of metabolic overheating and instead stimulate cellular preservation mechanisms (Figure 5). By restricting caloric intake to a shorter window of time, growth hormones like insulin and IGF-1 are activated, but to a lesser extent, reducing the risk of overweight, insulin resistance and, consequently, metabolic alterations favouring aging and the development of chronic diseases. Additionally, as mentioned before, the longer period of fasting forces the cells to enter maintenance mode and prioritize repairing and maintaining its structures over growth at all costs. At the molecular level, this results in the activation of sensors of the decrease in available energy (AMPK and sirtuins, in particular) and the entry into play of conservation processes such as the repair of proteins and DNA, the synthesis of new mitochondria (mitogenesis), the recycling of damaged components (known as the process of autophagy), and the renewal of stem cells.
It is important to mention that the benefits associated with intermittent fasting will be all the more evident if the energy consumed during the period of caloric intake comes mainly from plants. It has long been known that a plant-based diet (fruits, vegetables, legumes, nuts, seeds, etc.) provides a high intake of vitamins, minerals and certain bioactive compounds (polyphenols, for example), which have anti-inflammatory properties while being excellent sources of complex carbohydrates and unsaturated fats, nutrients that are essential for significantly reducing the risk of chronic diseases, especially cardiovascular diseases. It should also be mentioned that plant-based proteins, being less rich in methionine and branched-chain amino acids (BCAAs), activate GH/IGF-1 and insulin production less strongly than animal proteins and thus reduce the risk of insulin resistance and type 2 diabetes. Since the GH/IGF-1 pathway also represents a potent activator of mTOR (involved in protein synthesis and cell growth), the reduction of GH/IGF-1 by vegetable proteins helps to reduce the activity of this mTOR and thus stimulate autophagy, the recycling of cellular components essential to maintaining cell health.
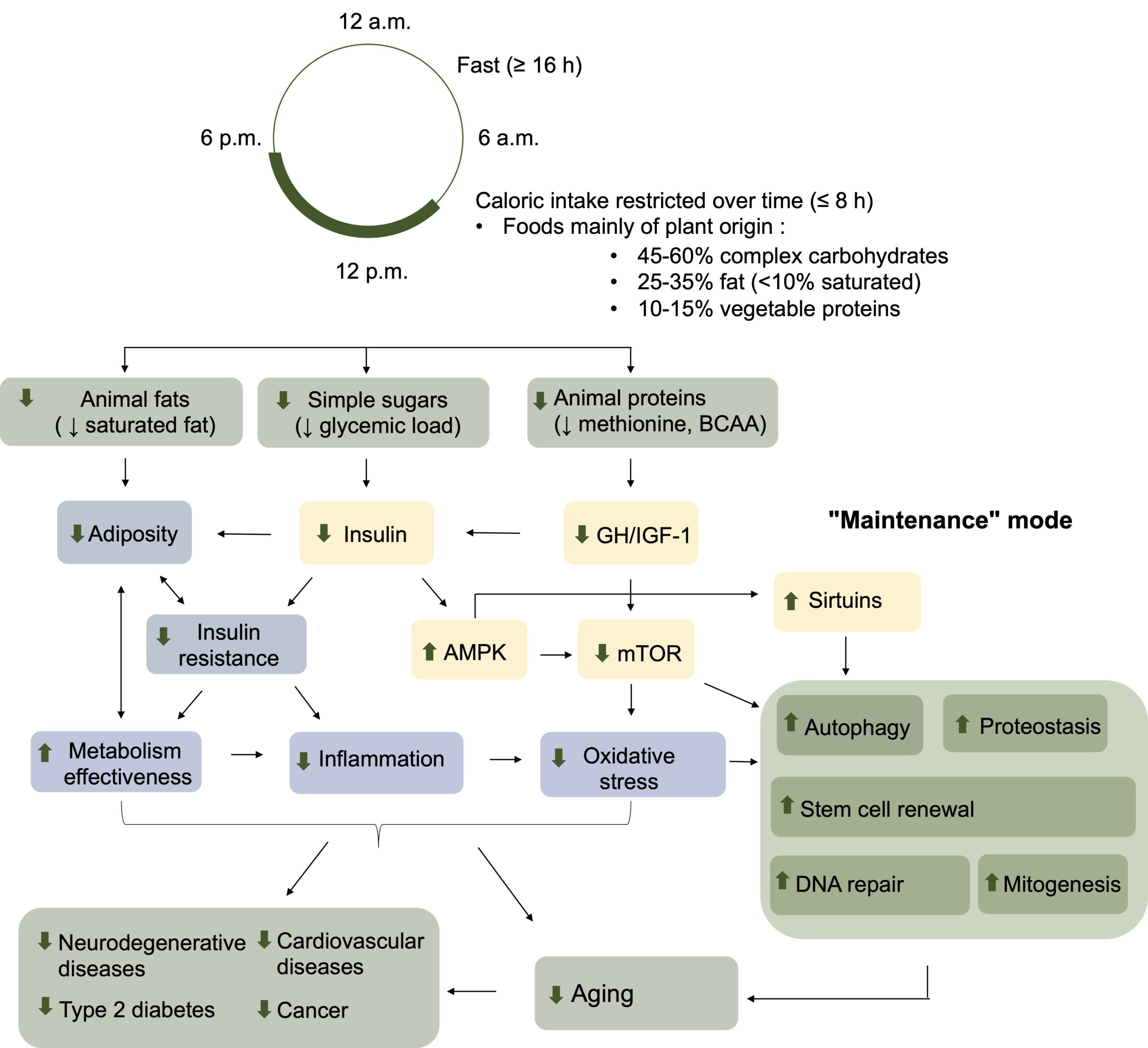
Figure 5. Metabolic and physiological impacts of time-restricted eating and a predominantly plant-based diet. A caloric intake restricted to a time window of less than 8 hours and composed of plant-based nutrients (complex carbohydrates, unsaturated fats, proteins low in methionine and branched-chain amino acids (BCAAs)) promotes low resistance to insulin, low adiposity, moderate levels of GH/IGF-1 activities, reduced mTOR signalling, and increased autophagy. The combination of these effects improves metabolic functioning, reduces inflammation and oxidative stress, and promotes the maintenance and repair of cellular functions, which can lead to a slowing of the aging process and a decrease in the incidence of several chronic diseases, including diabetes, certain cancers, cardiovascular diseases and neurodegeneration. Adapted from Longo and Anderson (2022).
In short, we can see TRE (and intermittent fasting as a whole) as a simple way to use evolutionarily selected mechanisms to our advantage to optimize the functioning of our metabolism and thus create conditions incompatible with the development of chronic diseases. We must realize that we are currently living in an era of unprecedented food abundance, for which our physiology, which has evolved to deal with the scarcity of food, is completely unsuited. Controlling caloric intake in such an environment is not easy, especially for people who are overweight and who are trying to lose weight by eating less. Indeed, low-calorie diets are most of the time ineffective in the long term, because caloric restriction is extremely difficult to sustain over long periods of time.
Restricting daily calorie intake to time windows shorter than 12 h, as with TRE, represents an attractive alternative to calorie restriction. On the one hand, it is not necessary to decrease the total amount of calories consumed to control weight, which makes this approach much more accessible for most people (in practice, studies indicate that people who adhere to TRE still decrease their calorie intake, but unintentionally). Additionally, intermittent fasting does not increase appetite hormones like ghrelin (unlike calorie restriction), which makes people less hungry and therefore less likely to “cheat” and abandon this approach.
In sum, TRE can be considered a form of “food self-defence” against the overabundance of calories present in our environment. By minimizing caloric excesses, this moderate and cautious approach helps to better control body weight and thus reduce the risk of all chronic diseases that result from being overweight.