Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesRespiratory infections are the most common type of infectious diseases and one of the leading causes of death worldwide. Different viruses (influenza, syncytial virus (RSV), rhinovirus, parainfluenza, metapneumovirus, adenovirus, and coronavirus) are the most common cause of respiratory infections in general, and are also the main culprits of pneumonia, the most serious type of infectious disease of the respiratory tract.
Several observations suggest a strong link between respiratory infections and the risk of cardiovascular events. For example, severe respiratory infections and acute coronary syndromes are known to exhibit similar seasonal variations, peaking in winter. Influenza epidemics have also been observed to be associated with increased morbidity (the number of people who become ill) and mortality from acute coronary syndromes, with up to half of the excess deaths occurring during these periods attributable to cardiovascular causes.
Studies that have examined this issue in more detail have confirmed this association; for example, it has been shown that up to one-third of acute coronary syndromes are preceded by a severe respiratory infection and that the risk of these serious cardiovascular events is five times higher in the week following the infection. Studies have also reported that this increased risk remains two to three times higher in the months that follow and can even persist for up to 10 years after hospitalization for pneumonia. It appears that older adults (65 years and older), as well as those with a history of cardiovascular disease or who are at high risk (type 2 diabetes, smoking, high cholesterol), are the most likely to develop cardiovascular complications associated with respiratory infections. It is therefore probable that these infections create conditions that promote the progression of pre-existing coronary artery disease, thereby increasing the risk of a cardiovascular event.
Systemic inflammation
How can a local infection in the lungs spread throughout the body and so significantly affect cardiovascular health? The answer lies in the highly aggressive immune response triggered by respiratory viruses, characterized by a high-intensity “cytokine storm” accompanied by an overactivation of blood clotting processes. Inflammatory molecules, initially present in the pulmonary infections, are taken up by the blood circulating in the lungs to be oxygenated and then ejected into the bloodstream by the contraction of the left ventricle of the heart (Figure 1). The inflammation then becomes systemic, meaning that all blood vessels are exposed to inflammatory stress. This is particularly true for the coronary arteries, which supply blood to the heart muscle cells, since these arteries represent the first branch of the aorta and receive approximately 5% of the cardiac output alone.
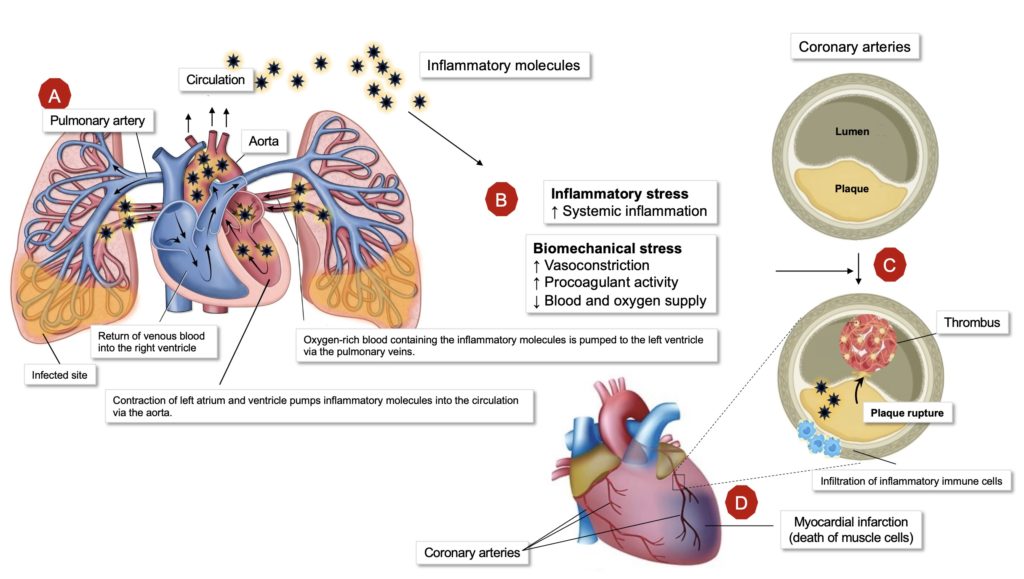
This exposure of the coronary arteries to the inflammatory stress resulting from infection can be problematic, as it is well established that inflammation plays a crucial role in the rupture of atherosclerotic plaques, responsible for approximately 70% of acute coronary syndromes. Studies show that the coronary arteries of individuals who have died from an acute viral infection exhibit a higher infiltration of pro-inflammatory immune cells, a class of cells that contribute to the development of acute coronary syndromes by producing various molecules (cytokines, proteases, free radicals) that increase vessel damage, weaken the fibrous cap that holds the plaques in place, and lead to thrombus (clot) formation(Figure 1C). Acute infections can also promote the development of these thrombi by directly activating platelets(aggregating effect = thrombus) as well as by causing coronary vasoconstriction which further narrows the lumen of the arteries and thus generates biomechanical stress on coronary plaques, which can cause their rupture.
Respiratory Syncytial Virus (RSV)
In addition to the well-established link between influenza virus infection and the risk of cardiovascular events, a recent study suggests that these events could also be significantly increased by RSV, another widespread respiratory virus. This highly contagious virus is particularly dangerous for young children and the elderly, especially those with chronic illnesses (cardiovascular and pulmonary diseases, type 2 diabetes, and asthma), and has a mortality rate similar to that of influenza. In this study, researchers used the Danish civil registry to identify 8,747 people with an average age of 71 who had been diagnosed with RSV infection between January 1, 2019, and December 31, 2024. These RSV-infected individuals were matched 1:1 with 8,747 uninfected individuals who had similar profiles (age, sex, and presence of various chronic diseases). For example, a 70-year-old woman with cancer at the time of RSV infection was compared to a woman of the same age who also had cancer but had not been infected. The incidence of serious cardiovascular events (myocardial infarction, stroke, and heart failure) and total events (including venous thrombosis, arrhythmias, and certain inflammatory diseases such as myocarditis) was subsequently compared between the two groups over a period of one year from the time of infection.
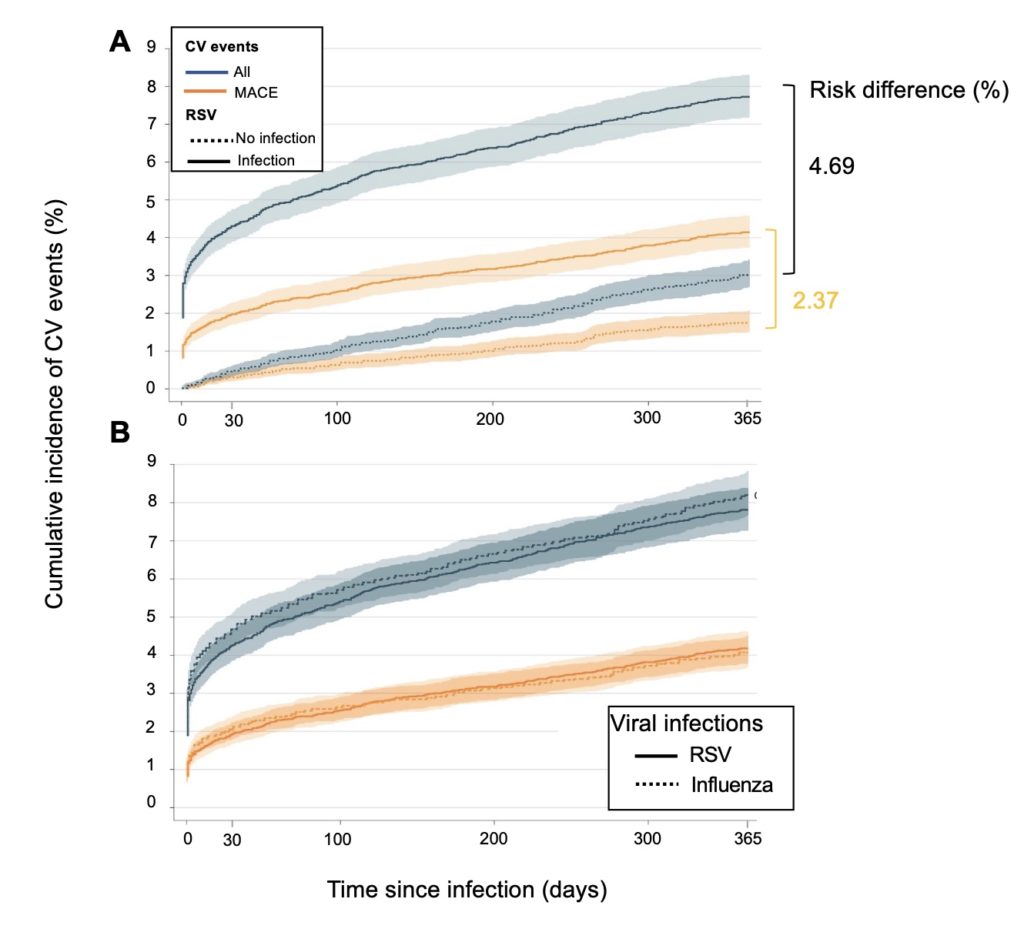
These comparisons clearly showed that the cumulative incidence of all cardiovascular events and major cardiovascular events was significantly higher in individuals infected with RSV than in uninfected individuals (Figure 2A). This increase in incidence is rapid, with a 3.8% and 1.6% increase in the risk of all and major cardiovascular events, respectively, within the first month, and remains elevated throughout the following year. This negative effect of RSV on cardiovascular health is of the same order of magnitude as that of the influenza virus (Figure 2B).
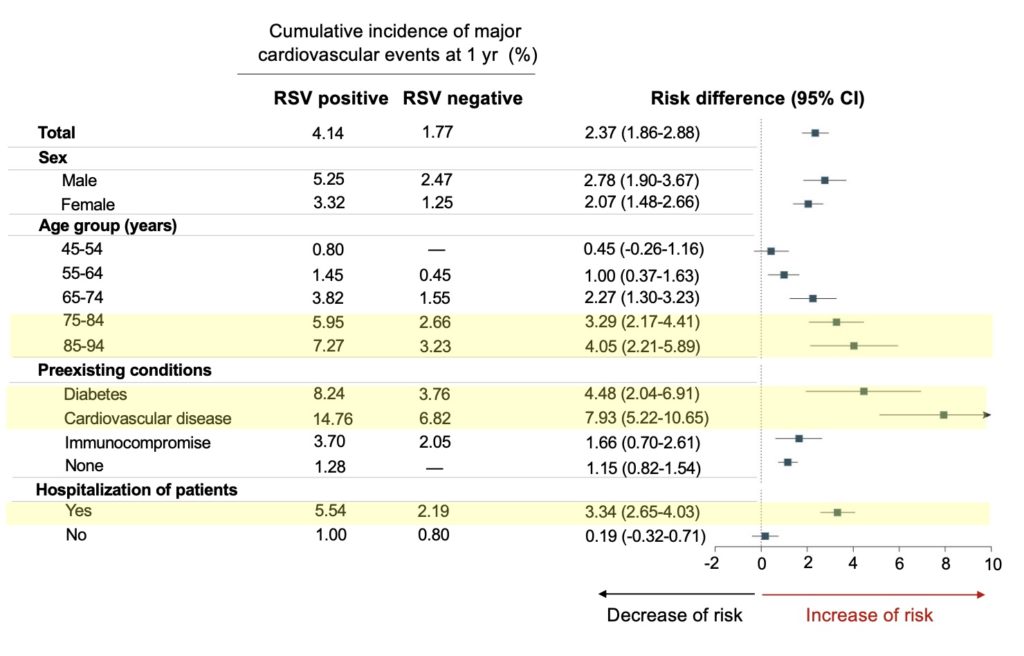
Further analysis shows that the risk of cardiovascular complications associated with RSV infection increases significantly in people aged 75 years and over, in those with cardiometabolic disease (type 2 diabetes, cardiovascular disease), as well as when the infection has required hospitalization of patients (Fig. 3).
The identification of a significant negative impact of RSV infection on cardiovascular health, comparable to that of influenza, underscores the importance of vaccination programs against this virus in vulnerable populations, such as the elderly or those at higher risk due to pre-existing cardiometabolic disease. These vaccines are now available (AREXVY and ABRYSVO) and can therefore not only reduce the burden associated with respiratory illnesses, but also mitigate the impact of RSV infection on the risk of subsequent cardiovascular disease.