Dr Éric Thorin, Ph. D.
Professeur titulaire, Département de Chirurgie, Université de Montréal. Chercheur au centre de recherche de l'Institut de cardiologie de Montréal.
See all articlesOverview
- The sugar we ingest is stored as fat—a survival mechanism that allows the body to store energy and release it when needed. Fat essentially acts like a battery.
- When this energy is not used, fat continues to accumulate. Fat cells (adipocytes) expand, leading to oxygen shortages and triggering stress responses that damage adipose tissue. This damage activates a local inflammatory response to “repair” the tissue.
- Inflammation—an energy-intensive process—interferes with normal fat metabolism and slows the uptake of blood glucose into storage cells, contributing to elevated blood sugar levels.
- To counteract this impaired glucose uptake and maintain stable blood sugar, the body produces more insulin.
- Insulin levels are elevated, but blood sugar remains normal: this defines insulin resistance.
- However, this compensatory mechanism has limits. If excess fat in adipocytes persists, the stress and inflammation continue.
- Over time, even higher levels of insulin are no longer sufficient to maintain normal blood sugar, which then begins to rise: this marks the onset of diabetes, characterized by elevated levels of both insulin and blood sugar.
- At this stage, sugar becomes particularly damaging: together with inflammation, it contributes to diseases of blood vessels, starting with the smallest ones, and leading to dysfunction in the brain, kidneys, heart, and eyes.
Insulin Resistance: A Metabolic Disorder
Insulin resistance is a metabolic disorder caused by excessive fat accumulation, especially abdominal fat. It is characterized by a gradual decline in the efficiency of mechanisms that regulate blood glucose. In the medium term, this dysregulation leads to diabetes, which is now widespread in Canada and globally. Diabetes lays the groundwork for both large-vessel diseases (e.g. atherosclerosis affecting the aorta, carotids, and coronaries) and small-vessel diseases affecting capillaries in all organs. By reducing oxygen supply to every cell, diabetes contributes to organ damage and diseases such as dementia, kidney failure, vision loss, and heart dysfunction. This article focuses on the causes of insulin resistance and its medium-term effects on cardiovascular health.
Normal Glucose Regulation
Under normal conditions, insulin maintains blood glucose at 4.8 mmol/L (about 0.8 g/L), which is equivalent to one teaspoon (5 g) of sugar in the entire bloodstream. After a meal, pancreatic beta cells detect rising glucose levels and release insulin. Insulin promotes glucose uptake into target organs—mainly muscles, fat tissue, and the liver. In the liver and muscles, glucose is stored as glycogen, which is later converted back to glucose during fasting to maintain blood sugar levels. Fat cells also store sugar as fat, which can be mobilized when needed. Fat (in the form of fatty acids) is the preferred energy source for muscles, including the heart, providing about 60% of daily caloric needs.
Basal energy expenditure (i.e. the energy required to stay awake while resting) ranges from 1600 to 1800 kcal/day for men and 1400 to 1600 kcal/day for women on average. You can calculate your basal metabolic rate using the Mifflin-St Jeor equation:
- For men: (10 × weight [kg]) + (6.25 × height [cm]) – (5 × age [years]) + 5
- For women: (10 × weight [kg]) + (6.25 × height [cm]) – (5 × age [years]) – 161
For example: A 63-year-old man weighing 75 kg and measuring 180 cm has a basal metabolic rate of 1,565 kcal/day. Glycogen stores alone can maintain blood glucose between meals. If levels drop too low, symptoms like dizziness and fainting can occur. When levels rise, insulin is released, and glucose is stored. Extra calories for physical activity come from fat stores. If unused (e.g. during prolonged fasting or exercise), fat remains stored.
Between meals, insulin plays a minor role. Other hormones mobilize energy:
- Glucagon stimulates glycogen breakdown (glycogenolysis) in response to low blood sugar.
- Adrenaline triggers fat release during exercise.
- Cortisol, the stress hormone, also mobilizes fat.
After 8+ hours of fasting, fat becomes the primary energy source. Triglycerides (three fatty acids bound to a glycerol) are released into the bloodstream. Cells break triglycerides into free fatty acids for energy, while glycerol is converted into ketone bodies, an alternative brain fuel because fatty acids do not enter the brain. Muscles and the heart, however, mainly use fatty acids. These fat “batteries” are discharged during physical activity or fasting.
Insulin Resistance: Driven by Inflammation
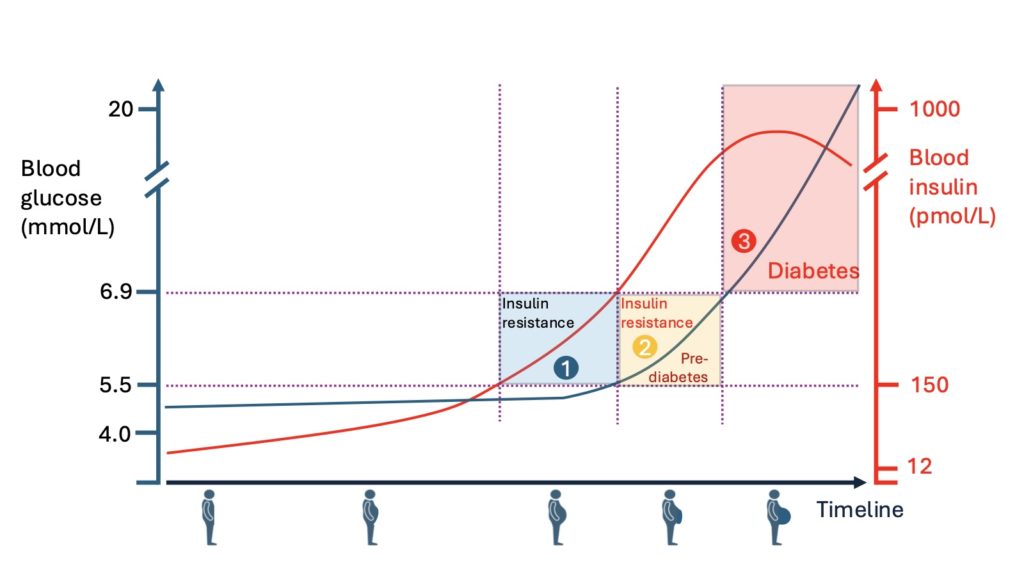
The first sign of glucose-insulin imbalance is insulin resistance, defined by elevated insulin levels with normal glucose (Fig. 1, square 1). This is usually triggered by fat accumulation—particularly abdominal. Enlarged adipocytes receive insufficient blood flow, leading to hypoxia and cell stress. This activates a repair response involving inflammation. Persistent inflammation is thought to reduce insulin efficacy. To maintain glucose at 4.8 mmol/L, insulin levels must increase further (Fig. 1, square 2).
Chronic Inflammation and Immune Activation
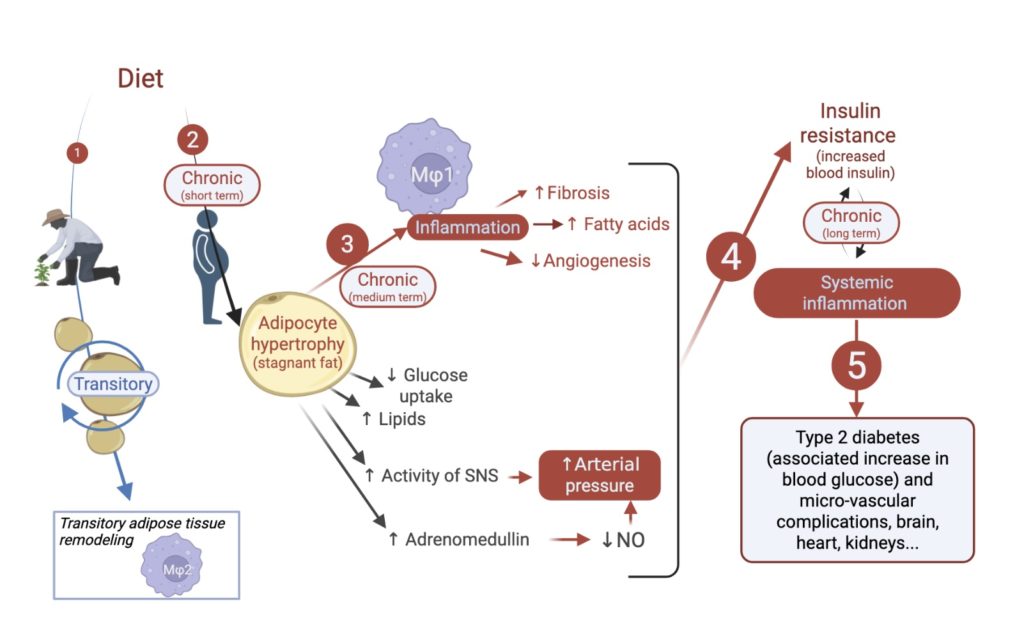
In hypertrophied adipose tissue, immune cells like type 1 macrophages and Th1 helper T cells infiltrate, releasing inflammatory cytokines (e.g. TNF-α, IL-1β, IFN-γ). Normally, type 2 macrophages dominate and support healthy, transient inflammation that promotes blood vessel growth (angiogenesis) and energy mobilization (Fig. 2). However, chronic fat overload sustains an inflammatory environment that spreads systemically, contributing to insulin resistance (Fig. 2). Though the exact molecular mechanisms remain under investigation, recent research has provided important insights.
Adipocyte Hypertrophy and Evolutionary Mismatch
Adipocyte expansion and contraction are natural and evolutionarily selected for energy storage during periods of food shortage (Williams, 1993). This process normally involves beneficial inflammation that helps with vascular remodeling and lipid mobilization. However, in high-income countries with continuous food access, fat accumulation often becomes chronic, decoupled from energy needs.
As a result, prolonged adipocyte hypertrophy leads to constant low-grade inflammation, which the immune system cannot resolve because its tools are geared toward eliminating infections or healing injuries—not resizing fat cells. Chronic inflammation becomes pathological, contributing to age-related diseases—a phenomenon known as inflammaging, the systemic, “cold” (non-infectious) inflammation that accelerates with obesity and insulin resistance.
The Damage Done by Sugar
This combination of insulin and high blood sugar, increasingly prolonged after each meal, will gradually damage our cells, starting with those of the blood vessels. Sugar will first deposit on the outer membrane of the cells lining the interior of the vessels—the endothelium. This single layer of cells is essential, forming the interface between the blood and the walls of all vessels (arteries, veins) and the cavities of the heart. The endothelium has anticoagulant, anti-adhesive, and vasodilatory properties. Given all these functions, it is easy to imagine that “caramelizing” it will lead to dysfunction, which will have major consequences on the regulation of blood flow to the organs, and in the long term, through a domino effect, on the very function of the organs themselves. Ultimately, blood supply will be reduced by the blockage of capillaries, the organs will become undernourished and in distress, and their cells (the functional units of each organ, each with a very specific role) will become stressed and damaged, eventually dying off one by one.
Reversing Insulin Resistance
Diabetes, an inevitable consequence of insulin resistance in the short or medium term, is—along with hypertension—one of the most dangerous risk factors for the cardiovascular system. In many cases, it is possible to reverse type 2 diabetes and drastically reduce the risk of cardiovascular complications associated with the disease (see our article on this topic). However, it is much simpler to act earlier and address insulin resistance before it progresses to type 2 diabetes. And this is indeed possible: as described in the previous section, the development of insulin resistance results from excess fat working in synergy with the inflammatory effects it causes. This means that this metabolic disorder can be reversed by eliminating the excess fat.
In other words, insulin resistance is a reversible condition, strongly influenced by lifestyle habits that promote weight gain—particularly poor diet and physical inactivity. To address it effectively, one must first understand that insulin resistance is an insidious condition. As previously mentioned, the main issues with detecting insulin resistance are that: i) insulin is not routinely measured, and ii) insulin resistance is usually only identified when fasting blood glucose exceeds 6.9 mmol/L (see Fig. 1, square 3).
However, insulin resistance actually begins when fasting insulin levels exceed 150 pmol/L while blood glucose is still maintained at 4.8 mmol/L (see Fig. 1, square 1). Therefore, measuring glucose alone is not very informative, as normal glucose levels may be associated with elevated insulin.
Broadly speaking, there are two conditions:
- Primary insulin resistance, when insulin levels rise to keep glucose normal;
- Secondary insulin resistance, when insulin, although elevated, can no longer maintain normal glucose levels.
In both cases, there is insulin resistance, but in the second, it becomes decompensated, leading to type 2 diabetes (Fig. 1, square 3). It is therefore important to emphasize the following: in order to distinguish between primary and secondary insulin resistance in an individual, insulin must be measured in addition to blood glucose. In other words, one cannot rely solely on fasting glucose levels to determine whether insulin resistance is present.
In practical terms, excess body fat—especially when located in the abdominal region—should be considered the main risk factor for developing insulin resistance. Consequently, insulin should be measured alongside glucose to provide objective evidence of this physiological imbalance and to strengthen preventive messaging. Reducing body fat, which is the source of inflammatory stimulus, is in fact the key to reducing inflammation and its long-term consequences. By eliminating primary insulin resistance without leaving a trace, the gateway to diabetes is effectively closed.
As the old saying goes, “an ounce of prevention is worth a pound of cure.” Identifying insulin resistance early in order to correct it as soon as possible (through healthy eating and regular exercise) appears to be the most sensible approach—both in older individuals and in children and adolescents. Given the sharp rise in overweight prevalence among young people, insulin resistance is appearing earlier and is causing catastrophic consequences for their health from the start of adulthood.