Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesOverview
- The 16:8 diet is a form of intermittent fasting in which food intake is restricted to an 8-hour window, alternating with 16-hour fasting periods.
- Two main types of 16:8 diets can be adopted, either by concentrating caloric intake early in the day, from 7 a.m. to 3 p.m. for example, or by skipping breakfast, with food intake limited to 12 p.m. to 7 p.m. for example.
- Studies show that both approaches lead to significant weight loss, but that caloric restriction early in the day provides greater metabolic benefits than restriction later in the day, possibly due to better synchronicity with circadian rhythms of metabolism.
- Despite this advantage, it can be difficult to reconcile this restricted eating window early in the day with one’s family, social, and professional life.
- Ultimately, both approaches have their advantages and disadvantages and adopting one or the other comes down to choosing the one that fits most easily into daily life.
Intermittent fasting has become an approach used by more and more people to lose weight in recent years. One of the reasons for this popularity is its great simplicity: it only involves alternating periods of eating with periods of fasting that can vary in length, without necessarily having to avoid specific food groups or macronutrients (as in keto or very low-fat vegan diets) or carefully monitor daily calories.
There are three main types of intermittent fasting: 1) alternate day fasting, where one fasts every other day, either by consuming only water or by restricting caloric intake to approximately 25% of their needs (500-800 kcal); 2) the 5:2 diet, which involves 5 days of normal caloric intake and 2 days of fasting (consecutive or not) per week; and 3) time-restricted feeding (TRF), where caloric intake is restricted to a certain time of the day, 3-5 days per week. Regardless of the type of intermittent fasting adopted, studies show that this form of dietary restriction reduces body weight, improves glucose tolerance, protects against hepatosteatosis, reduces atherogenic lipids and blood pressure, and improves gut function and cardiometabolic health.
TRF is probably the easiest form of intermittent fasting to adopt because the fasting periods are much shorter than in other types of intermittent fasting. In practical terms, this means that instead of eating all meals during a 12-14 hour window and sometimes even longer (as is the case for most people in North America), for example from 6 a.m.-7 a.m. in the morning until 7 p.m.-8 p.m. in the evening, food intake is restricted to a smaller window, generally 6 to 8 hours (Figure 1). This time limit can be respected in two main ways: either by eating breakfast and dinner early (7 a.m.-3 p.m., for example) or by skipping breakfast and eating dinner later (11 a.m.-7 p.m. for example).
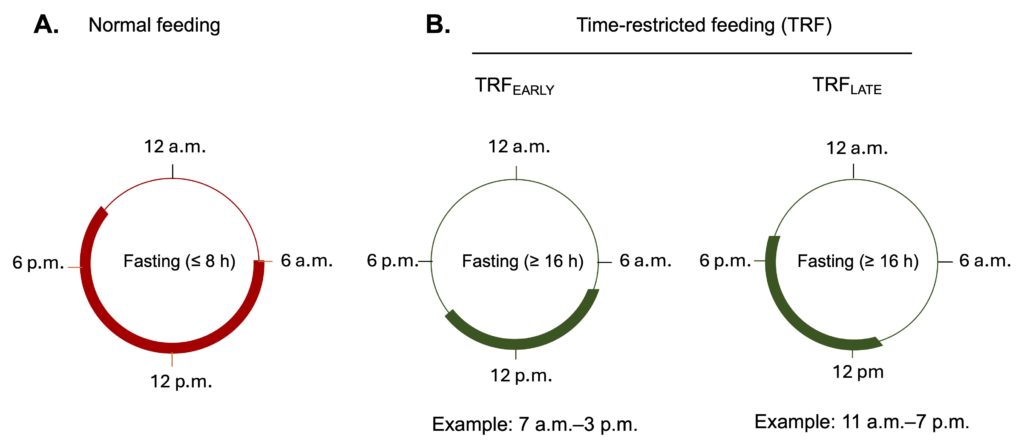
Figure 1. Schematic representation of the concept of time-restricted feeding (TRF). Unlike the standard diet, where calories are typically consumed over a period of 12 hours or more (red line), caloric intake is reduced to a 6–8-hour window in TRF (green lines), which allows for a significant increase in the duration of the fasting period. Two main types of TRF can be distinguished depending on the period in which this caloric intake is concentrated, either at the beginning (TRFEARLY) or at the end of the day (TRFLATE).
Studies show that TRF is generally associated with a small but significant weight loss, in the range of 1-4% in overweight or obese subjects, as well as a decrease in waist circumference (a marker of abdominal obesity). These losses are mainly due to an unintentional reduction in caloric intake, of 10-30% (200-600 kcal/day) depending on the study (see here, for example). These benefits are greater than those observed in people who reduce their overall caloric intake, but without limiting food consumption to a defined portion of the day, as is the case in TRF. It should be mentioned, however, that TRF could reduce the risk of cardiometabolic diseases by improving several physiological parameters such as insulin sensitivity, oxidative stress, blood pressure, and pancreatic function, even in the absence of significant weight loss.
It seems that it is not only what we eat that influences our health, but also when we eat it. According to the new concept of “chrononutrition,” it is possible to optimize the efficiency of the metabolic response to what we eat by limiting caloric intake to a specific time of day, so that it is synchronized with the cycles of our biological clock (circadian rhythms).
Circadian rhythms
Circadian rhythms are regular fluctuations, over a period of approximately 24 hours, of a certain number of physiological processes essential to the functioning of the body. The production of hormones such as melatonin, cortisol, insulin, or even certain enzymes (those involved in digestion, in particular) is governed by these circadian rhythms, which makes it possible to optimize metabolism by using the energy available during the waking period (catabolism) while storing the excess during the sleeping period for future use (anabolism) (see our article on this subject).
This is particularly striking with regard to glucose metabolism: several studies have indeed shown that insulin sensitivity and glucose tolerance are at their peak during the morning and decrease significantly thereafter. As a result, when meals are consumed late in the evening (when the insulin production cycle is at its lowest due to the inhibitory effect of melatonin), there is an increase in blood glucose, as well as an increase in appetite and the risk of obesity. Several studies have shown that this type of desynchronization between food intake and the normal cycle of circadian rhythms, for example in night workers or in people who eat irregularly (>5 meals per day), increases the risk of cardiometabolic diseases by disrupting the control of sugar and fat metabolism, blood pressure, and body weight. Conversely, restricting caloric intake to a certain period of the day, as in intermittent fasting, facilitates the balance of these rhythms and improves metabolism by positively influencing the activity of metabolic sentinels such as AMPK and mTOR (see our article on this subject).
TRF Early or Late?
Currently available evidence suggests that different forms of TRF, whether early or late in the day, improve metabolic health by reducing caloric intake, decreasing body weight and blood pressure, and improving insulin sensitivity.
However, if eating early in the day can synchronize caloric intake with the fluctuations dictated by our biological clock and thus optimize the metabolic response to the food consumed, does this mean that the benefits observed in TRF studies might be even more pronounced in those who practise TRFEARLY than in those who adopt TRFLATE?
Few studies have directly compared the effects of these two feeding windows, but currently available data suggest a slight advantage for an early day food intake. For example, one study examined changes in several cardiometabolic risk factors in approximately 40 overweight adults (mean BMI of 28) who were randomized to two TRF groups: TRFEARLY (meal intake between 7 a.m. and 1 p.m.) and TRFLATE (meal intake between 12 p.m. and 6 p.m.) (Figure 2). Both types of TRF resulted in equivalent weight loss (approximately 4% of baseline weight), but the benefits of TRF on fasting insulin levels, insulin resistance, and blood pressure were more pronounced in volunteers whose caloric intake was restricted to the morning. One of the biggest differences is the marked drop (nearly 6 mmHg) in systolic blood pressure following 8 weeks of the TRFEARLY diet, a decrease of the same order of magnitude as that observed with an antihypertensive drug.
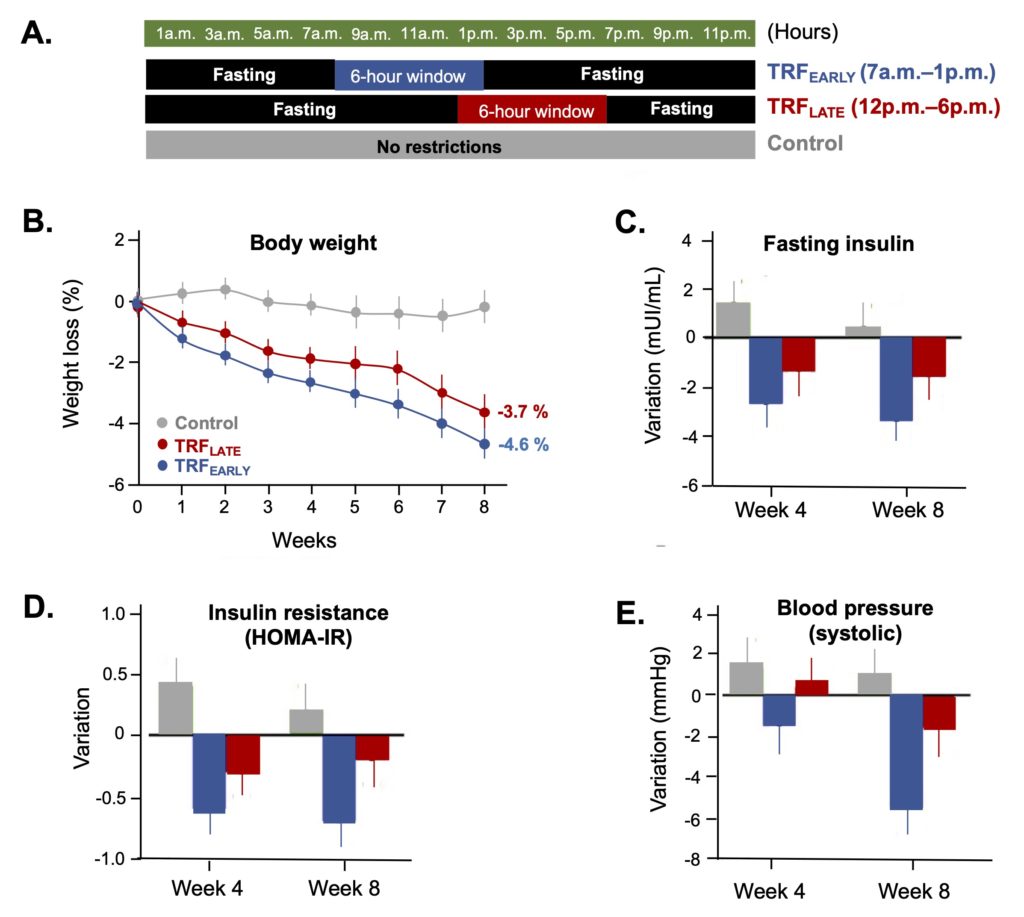
Figure 2. Effects of two types of time-restricted feeding on cardiometabolic disease risk factors. A. Schematic representation of the two experimental protocols tested in the study, TRFEARLY (7 a.m.-1 p.m.) and TRFLATE (12 p.m.-6 p.m.). B-E. Comparison of the effects of the two types of TRF on body weight, insulin levels, insulin resistance, and blood pressure. Note that while both types of TRF induce similar levels of weight loss, the positive effects of TRFEARLY are more pronounced regarding the different risk factors. From Zhang et al. (2022).
These differences in responses are not, however, systematically observed in all studies. For example, when comparing the cardiometabolic effects of the two feeding windows (8 a.m.-4 p.m. vs. 12 p.m.-8 p.m.) combined with a 25% reduction in caloric intake, another study did not observe significant differences, whether in terms of weight loss (−4.2 vs. −4.8 kg), fat mass (−2.9 vs. −3.6 kg), or fasting glucose (−4 vs. −2 mg/dL). Another study showed that TRF improved glycemic control in obese individuals at high risk of type 2 diabetes and that this improvement was similar for TRFEARLY (8 a.m.-5 p.m.) and TRFLATE (12 p.m.-9 p.m.).
In sum, it appears that caloric restriction, whether early or later in the day, leads to small but significant weight loss, possibly due to an unintentional reduction in energy consumption. Given that excess weight is a major risk factor for cardiometabolic diseases, either of these two restricted eating windows may therefore help reduce the negative effects of being overweight. In several (but not all) studies, TRFEARLY appears to be more effective than TRFLATE in improving other cardiometabolic disease risk factors such as blood pressure, blood glucose, and insulin resistance. This superior effect of an early-day eating window is biologically plausible, given that the circadian rhythms of the processes that govern glucose metabolism function optimally in the morning.
Breakfast, an essential meal?
Another reason often given for favouring time-restricted eating at the beginning rather than at the end of the day is the omission of breakfast by people who adhere to TRFLATE. One of the dogmas of modern nutrition is that breakfast is a very important meal (and even the most important of the day, according to some) and that there would therefore be negative consequences to skipping this meal.
This emphasis on the importance of breakfast comes largely from population studies reporting an association between skipping breakfast and an increased risk of obesity, type 2 diabetes, cardiovascular disease, and premature mortality. However, some studies have suggested that people who do not eat breakfast are at increased risk of cardiometabolic diseases only if skipping breakfast is combined with a habitual late-night meal consumption. Moreover, some studies have observed that skipping breakfast without eating late the night before was not associated with a marked increase in the risk of obesity, blood glucose abnormalities, or poor metabolic health in general. Since people who adopt a time-restricted diet where the last meal is consumed early (before 7 p.m.) generally lose weight and improve their glucose metabolism, it is unlikely that skipping breakfast a few days a week could have consequences as negative as those reported by population-based studies.
Breakfast and body weight control
This seems particularly the case with regard to the link between obesity and the absence of breakfast that is systematically observed in these studies. Given that excess weight is due to an excessive energy intake, it has been proposed that the lower incidence of obesity in people who eat breakfast daily is related to a lasting satiety effect associated with breakfast, i.e. eating early in the day would allow better control of appetite throughout the day and thus avoid an excessive energy intake leading to overweight.
However, when this hypothesis has been rigorously tested in randomized clinical trials, skipping breakfast has not been found to increase appetite at subsequent meals and has been found to have no impact on total caloric intake. In other words, there is no causal relationship between skipping breakfast and the risk of becoming obese. In fact, a meta-analysis of several randomized trials on this topic showed that overall, people who skip breakfast consume fewer calories during the day (about 260 kcal/d) and even lose slightly more weight compared to those who eat breakfast. This is consistent with a study of 50,660 adult members of Seventh-day Adventist churches showing that one or two meals per day were associated with a lower BMI than three meals per day. In short, whether or not to eat breakfast probably has no major impact on body weight and it is therefore likely that the association between the incidence of obesity and the absence of breakfast observed in epidemiological studies is indirect, i.e. that it rather involves external factors (see below) which confuse the issue by simultaneously influencing the two parameters measured (obesity and breakfast). These confounding factors are inseparable from population-based studies and remain extremely difficult for researchers to control.
Breakfast and cardiovascular disease
The increased risk of cardiovascular disease and premature mortality observed in those who regularly skip breakfast is a good example of the contribution of these confounding factors. This negative impact on heart health initially stems from a Harvard University study of 26,902 health professionals, which found that people who consistently skipped breakfast had a 27% increased risk of coronary heart disease compared to those who ate breakfast every day. Other studies have come to similar conclusions (see here, here and here), so much so that the AHA’s official recommendation is to eat breakfast every day to reduce the risk of cardiovascular disease.
It should be noted, however, that this association appears to be due in large part to an increase in certain cardiovascular risk factors in people who never eat breakfast, such as overweight, hypertension, hypercholesterolemia, and type 2 diabetes. Given that the increased risk of overweight in people who skip breakfast is not observed in randomized studies (see previous section), it is therefore possible that the increased risk of cardiovascular disease caused by excess weight still involves the contribution of confounding factors.
This is highlighted by the results of another study that examined the impact of breakfast consumption on the risk of premature mortality (all cause and cardiovascular) in 6,674 adults aged 40 to 75. The researchers observed that people who never ate breakfast had an 87% increased risk of cardiovascular mortality (RR=1.87), mainly due to a marked increase in the risk of stroke (Figure 3). However, in this study (as in most of those that have reported an increase in cardiovascular risk), the subjects who skipped breakfast were also those who had several baseline characteristics known to significantly increase the risk of premature mortality (smoking, excessive alcohol consumption, obesity, type 2 diabetes, high cholesterol, physical inactivity, poor diet quality, and low socioeconomic status). Although the authors used statistical models meant to attenuate the influence of these factors, it remains almost impossible to completely eliminate their contribution to the results obtained. In other words, skipping breakfast would not be an independent risk factor for premature mortality, but rather a marker of poor lifestyle habits in general, particularly in terms of diet and physical activity, which are well known to increase this risk.
In the context of a time-restricted diet, it is also important to mention that a significant increase in the risk of premature mortality is only observed in people who never eat breakfast (Figure 3). Since TRF is generally practised 3-5 days a week, simply eating breakfast occasionally would therefore completely cancel out this increased risk.
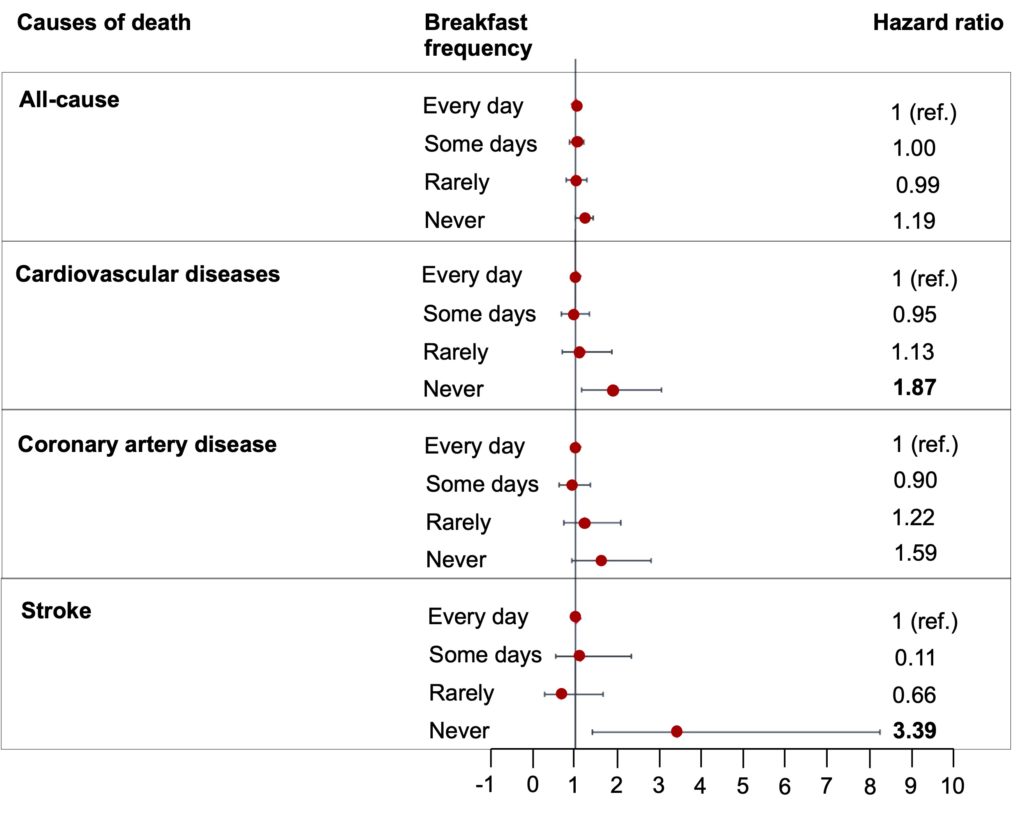
Figure 3. Relationship between the risk of premature mortality from any cause or cardiovascular disease and the frequency of breakfast consumption. N.B. Bold numbers indicate an increased risk that is statistically significant. Adapted from Rong et al. (2019).
A question of feasibility
Going back to the initial question: is it better to extend the fasting period by eating early dinner or by skipping breakfast? In both cases, studies show a clear improvement in body weight and metabolism (glycemia, insulin sensitivity), but it seems that the metabolic effects are more pronounced when caloric intake is concentrated early in the day (TRFEARLY), quite possibly due to better synchronicity with the circadian rhythms of metabolism. Studies show that this type of TRF is generally well tolerated and, in some cases, is accompanied by a notable improvement in the mood and energy level of participants. However, these studies are short-term (usually a few weeks), and long-term adherence to this form of dietary restriction remains uncertain given that for the majority of people, regularly eating very early dinner (before 3 p.m.) is totally incompatible with their work, family and social life. In Western culture, dinner is usually the main meal of the day (about 35% of daily calories), and among TRF practitioners, most people (75%) prefer to maintain the routine surrounding this meal to preserve a “normal” social and family life by restricting their caloric intake in the middle rather than at the beginning of the day.
Each time-restricted eating pattern therefore has advantages and disadvantages, and the main factor that may dictate the adoption of one or the other is its feasibility, i.e. it is simply a matter of choosing the one that fits most easily into daily life. For people with more flexible schedules, an intermediate approach of TRF with a window from 10 a.m. to 5 p.m. could represent an interesting compromise, especially since a study has shown that this eating window improves glycemic control. Otherwise, a TRFLATE, from 12 p.m. to 7 p.m. for example, remains an interesting choice given its positive effects on the control of body weight and several metabolic parameters.