Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesOverview
- A large number of studies have shown that moderate alcohol intake causes a series of physiological changes that significantly reduce the risk of coronary heart disease and premature mortality.
- At higher doses, however, alcohol increases the risk of several diseases, particularly cancers of the upper digestive tract, and increases the risk of mortality.
- Several studies suggest that this increase in the risk of cancer and mortality is less pronounced among red wine drinkers.
- For people who drink alcohol, moderate consumption of red wine could therefore represent the best way to benefit from the positive effects of low doses of alcohol, while minimizing its negative effects.
As we mentioned in a previous article, an impressive number of population-based studies have reported a decreased incidence of cardiovascular disease, particularly coronary heart disease like myocardial infarction, in people who drink moderate amounts of alcohol. An overwhelming proportion of these studies in fact show a J-curve type relationship between the incidence of these diseases and alcohol consumption, i.e., that compared to non-drinkers, a moderate intake of alcohol (1 drink per day for women, 1-2 drinks per day for men) reduces the risk of coronary heart disease and premature mortality, but this protection disappears quickly at higher quantities, beyond 2 drinks per day for women and 4 glasses per day for men (Figure 1). Meta-analyses of hundreds of studies that have documented this phenomenon (see here and here, for example) show that the positive effect of low amounts of alcohol on mortality risk is primarily due to a reduction of 25% of the incidence and risk of mortality linked to cardiovascular disease, in particular coronary heart disease, compared to abstainers. It is important to mention that while the majority of studies that have looked at the link between moderate alcohol consumption and the reduction in the risk of mortality were carried out in the 1980s and 1990s, these results were confirmed by recent large-scale studies and can be considered a scientifically well-established fact.
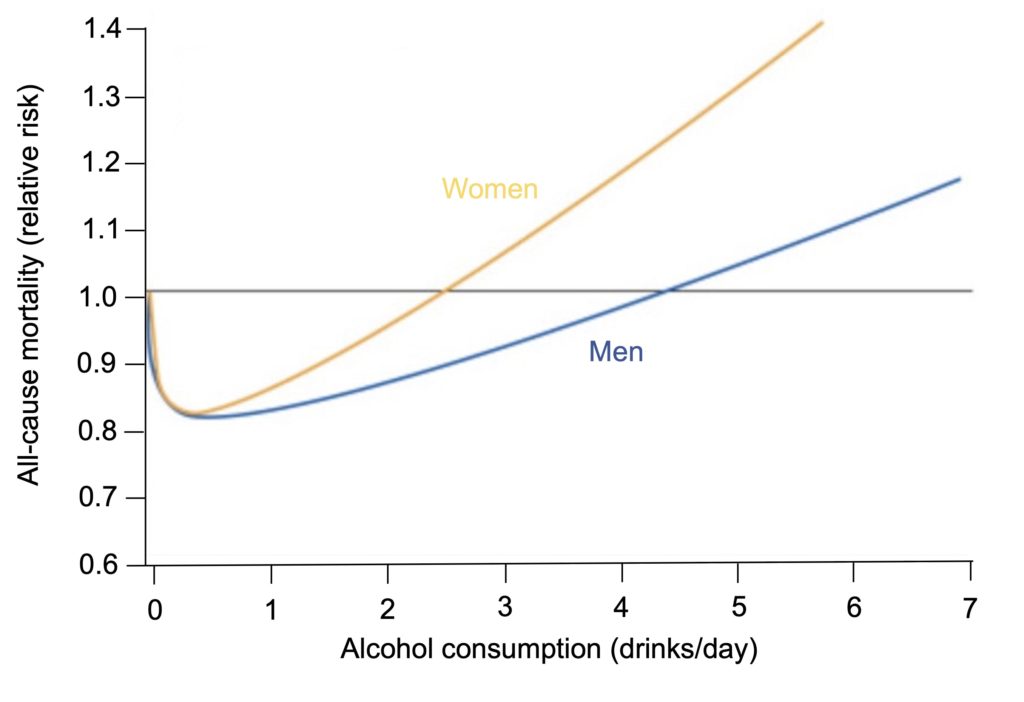
Figure 1. Example of the J-shaped relationship between mortality risk and the daily amount of alcohol consumed.This figure comes from a meta-analysis of 34 prospective studies, involving more than 1 million participants. Note that moderate alcohol intake (1 drink for women, 1-2 drinks for men) reduces the risk of premature mortality by approximately 18%. Adapted from Castelnuovo et al. (2006).
This biphasic “J” relationship between alcohol and mortality risk is largely explained by the increased risk of several diseases observed in the heaviest drinkers, notably cancers of the upper digestive tract (mouth, pharynx, larynx, esophagus) and liver cirrhosis, which cancel out the positive effects of alcohol on the risk of coronary heart disease (Figure 2). However, since cardiovascular disease, and in particular coronary artery disease, is one of the main causes of premature mortality, the cardioprotective effect of alcohol plays a central role in the reduction in mortality observed in population-based studies.
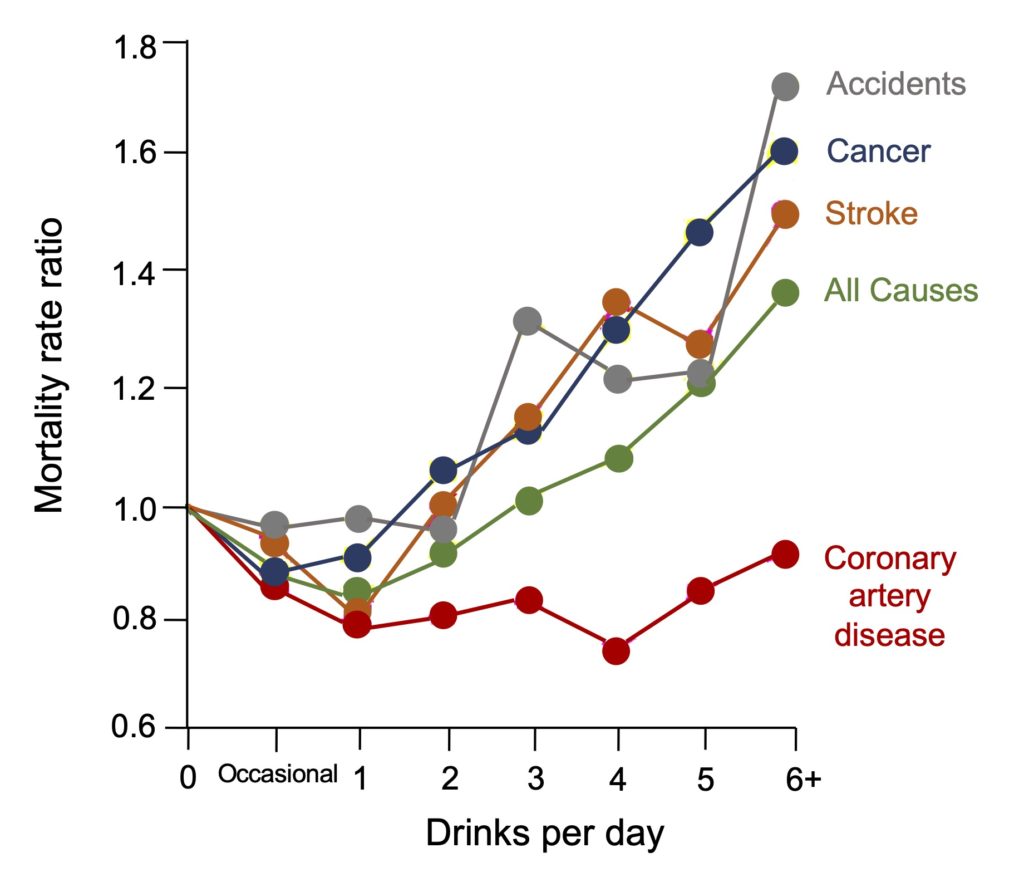
Figure 2. Variation in rates of different causes of mortality according to the daily amount of alcohol consumed.Note that coronary artery disease is the main cause of mortality positively influenced by alcohol consumption. Alcohol also reduces the risk of stroke mortality at low doses (especially in the form of red wine), but this effect disappears quickly at higher doses, likely due to the well-documented increase in blood pressure in heavy drinkers, a major risk factor for stroke. From Vogel (2002).
It is important to note that these beneficial effects of moderate quantities of alcohol on the risk of heart attack have been systematically observed in ALL large-scale studies carried out over the last 50 years, including the most recent ones that question the benefits of low-dose alcohol. In these studies, the cardioprotective effect of low doses of alcohol is indeed observed, but seems much weaker due to the authors’ choice to compare moderate drinkers to very light drinkers rather than to lifelong abstainers, as is generally the case in studies on alcohol (ex-drinkers were initially included in this group, but this practice has long since ceased, because stopping alcohol is often a sign of an underlying health condition) (Figure 3). In other words, by modifying the reference group in this way, the benefits on heart attack prevention are greatly attenuated and those on all-cause mortality are abolished, which could suggest that there is no benefit associated with even moderate consumption of alcohol. Yet, when these same studies use lifelong abstainers as a comparison scale, they also observe a reduction in the risk of cardiovascular disease and premature mortality, followed by a rapid increase in risk at higher levels of consumption (Figure 3).
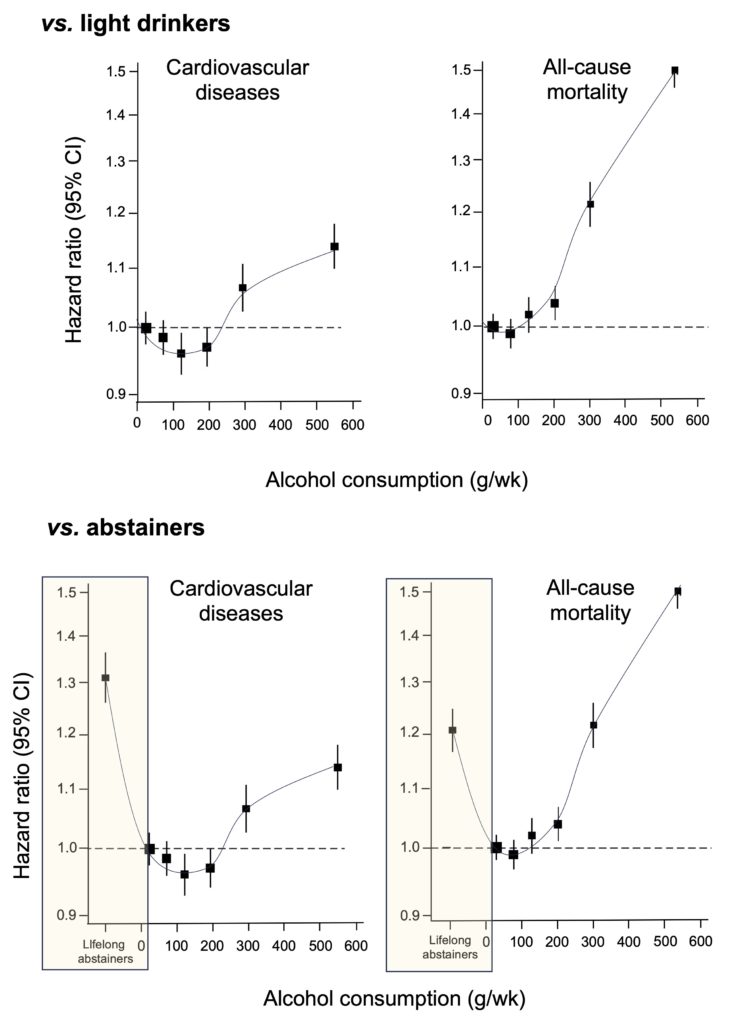
Figure 3. Variations in the interpretation of the effects of alcohol on the risk of cardiovascular disease and mortality depending on the group used as a reference. When very light drinkers (<25 g per week, or approximately 1-2 drinks) are used as a reference group (hazard ratio =1.0), the cardiovascular benefits of low amounts of alcohol are significantly attenuated and those on all-cause mortality disappear completely, which is interpreted by the authors as an indication that there is no benefit associated with alcohol consumption, even when it is moderate. However, if we use lifelong abstainers as a reference (yellow rectangles), as is normally the case in most studies (data not presented in the article, but included in the additional data available online), the figure clearly shows a strong reduction in the risks of cardiovascular disease and premature mortality, which takes the shape of a J-curve similar to that highlighted by hundreds of studies on the subject. Adapted from Wood et al. (2018).
The recent report from the CCSA (Canadian Center on Substance Use and Addiction), which was widely discussed last year and suggests the government drastically lower the quantities of alcohol recommended to the population, is almost exclusively based on this type of study using light drinkers rather than abstainers as the reference group. Although this approach can be useful in raising awareness of the risks that arise from excessive alcohol consumption, it has the disadvantage of brushing aside the well-documented positive effects that are associated with light or moderate consumption.
In sum, an unbiased reading of the research of the last 50 years leads to the conclusion that if the negative effects associated with excessive alcohol consumption are indisputable, so are the positive effects of moderate consumption, particularly with regard to the prevention of myocardial infarction. This cardioprotective effect of low-dose alcohol is part of the lifestyle habits associated with a reduction in the risk of premature mortality identified in several epidemiological studies and can certainly contribute to an optimal lifestyle for maintaining good health: for example, studies carried out in Sweden and the United States show that when combined with a healthy diet, regular physical activity and body weight control, moderate alcohol intake is one of the factors associated with a very significant reduction in the incidence of coronary heart disease and a spectacular increase (14 years) in life expectancy. It should also be noted that the cardioprotective effect of moderate alcohol consumption is also observed in people with a history of cardiovascular events. For example, a French study showed that among heart attack survivors, moderate wine consumption (2-4 glasses per day) was associated with a reduction in the risk of cardiovascular complications of the same order as that observed in healthy people. An Italian study came to the same conclusions, noting a 13% reduction in the risk of recurrence of cardiovascular events and a 23% reduction in the risk of all-cause mortality in coronary patients who drink wine moderately.
Cardioprotective mechanisms
A very large number of studies have examined the mechanisms involved in reducing the risk of cardiovascular disease, and more specifically myocardial infarction, associated with moderate consumption of alcoholic beverages (Figure 4). In addition to certain hormonal and metabolic effects that arise from alcohol (anti-inflammatory effect, improvement of insulin sensitivity, reduction of abdominal obesity (especially for red wine), improvement of endothelial function), two major biological effects identified so far seem particularly important for reducing the risk of coronary heart disease:
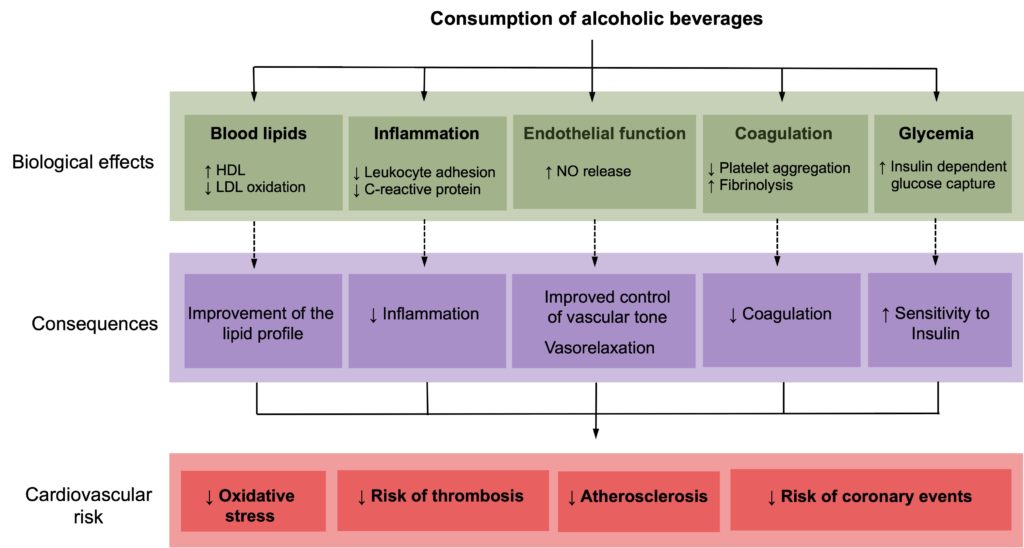
Figure 4. Proposed mechanisms for the reduced risk of cardiovascular diseases associated with moderate alcohol consumption. Adapted from Haseeb et al. (2017).
Improved lipid profile. Studies consistently observe an increase (around 10%) in blood levels of HDL cholesterol and apolipoprotein AI (a major structural protein of HDLs) associated with moderate alcohol intake (2 drinks per day). HDL particles are involved in the transport of cholesterol from the arteries to the liver, which helps reduce the development of atherosclerosis (this is why HDLs are commonly referred to as “good” cholesterol), and a very large number of studieshave shown that an increase in HDL is associated with a significant reduction in the risk of coronary heart disease. There is therefore little doubt that this increase in HDLs contributes to the cardioprotective effect observed in moderate alcohol drinkers. Based on available data, it is estimated that approximately 30% of the reduction in cardiovascular disease risk observed in moderate drinkers is due to this improvement in the lipid profile. All types of alcoholic beverages raise blood HDL levels, but some studies have suggested that this increase may be more pronounced in moderate wine drinkers. Red wine (but not other types of alcohol) is also associated with a reduction in the oxidation of LDL particles (a key phenomenon in the development of atherosclerosis), a biological activity due to its polyphenol content (discussed below, see Figure 6).
Anticoagulant effect. The reduced risk of thrombosis (clot formation) also appears to play a central role in the positive effects of moderate alcohol consumption on the risk of heart attack. Several randomized studies have clearly shown that at low doses, alcohol lowers blood levels of fibrinogen (the protein used to form clots) and at the same time increases levels of tissue plasminogen activator (tPA), an enzyme that dissolves these clots. Platelet aggregation (the initial stage of blood clotting) was also found to be significantly reduced in moderate drinkers, particularly red wine drinkers. It has been proposed that this phenomenon could contribute to the low incidence of coronary mortality observed in France compared to several other countries, despite a diet very rich in saturated fat and high blood cholesterol levels. Although it is unlikely that this “French paradox” is entirely attributable to red wine consumption (other dietary factors are certainly at play), these observations have nevertheless led to a considerable number of studies aimed at determining whether moderate consumption of red wine could provide more health benefits than other types of alcoholic beverages.
Red wine, a complex alcoholic drink
Traces of winemaking have been found in Georgia (South Caucasus) dating back about 8,000 years, making wine the oldest alcoholic beverage consumed by humans. Wine is also distinguished from other types of alcohol by its greater molecular complexity, with the presence of at least 500 distinct phenolic compounds, present in the original grape and extracted during the fermentation process (Figure 5). Although quantitatively scarce (less than 1% of the constituents of wine), these phenolic compounds give the wine its unique organoleptic properties, both in terms of colour, taste and mouthfeel.
During winemaking, pressing (separation of the juice and grape skins) occurs before fermentation for white wine, but after for red wine. Since these phenolic compounds mainly come from the grape skins, prolonged contact with the skins during fermentation allows better extraction of these molecules, hence their presence in much greater quantities in red wine than in white wine (Figure 6).
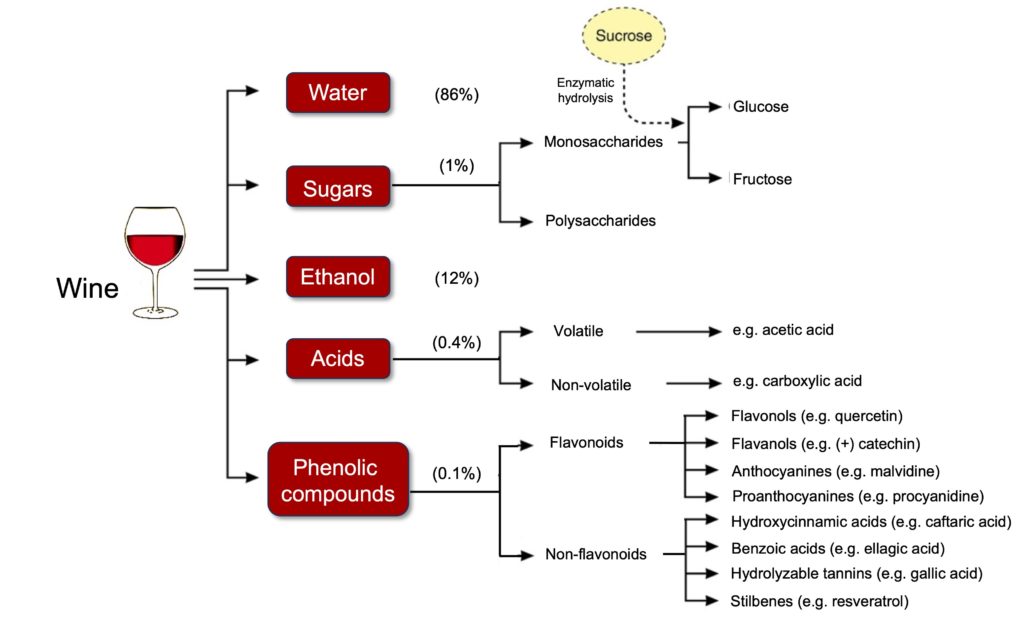
Figure 5. Overview of the chemical composition of wine. Adapted from Haseeb et al. (2017).
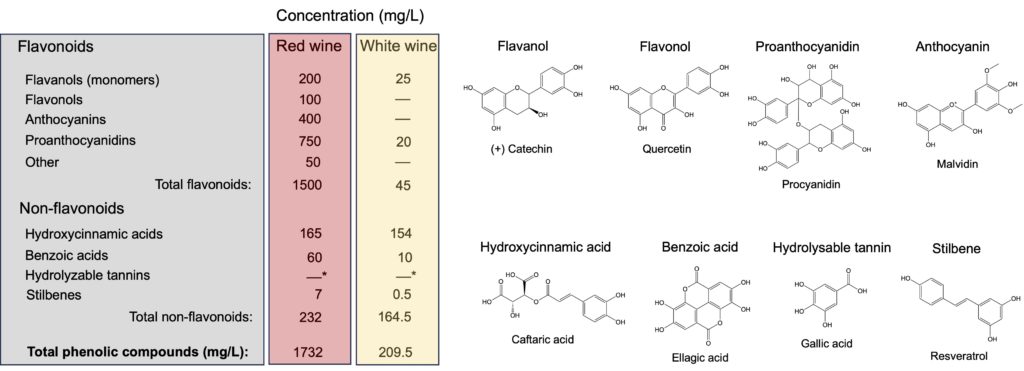
Figure 6. Phenolic compound content of red and white wines. Note that these concentrations vary enormously depending on the grape variety, the geographical location of the vines, the climate, and the different processes used to make the wines. *Hydrolysable tannins come from the oak barrels used to age certain wines, and their quantities therefore depend on the time in wooden barrels. Waterhouse (2002).
Beyond their importance in the structure of wine, phenolic compounds could also contribute to the positive effects of moderate wine consumption observed in epidemiological studies. It is well established that a high dietary intake of polyphenols, in particular those of the flavonoid class, is associated with a significant reduction in the incidence of cardiovascular events (see here and here, for example). In addition to containing several flavonoids found in commonly consumed fruits and vegetables (e.g., quercetin, catechin, ellagic acid), red wine also represents the only significant dietary source of resveratrol, a phenolic compound that is extracted from grape skins during fermentation. This molecule could play a central role in the cardioprotective effects of red wine given its numerous biological activities at the vascular level, including an increase in production of the vasodilator NO (nitric oxide) and a reduction in oxidative stress and inflammation.
Although resveratrol and polyphenols in general are quantitatively scarce in red wine, several observations suggest that these biological activities (antioxidant, anti-inflammatory, vasorelaxant) probably contribute to the cardioprotective effect associated with moderate consumption of red wine:
- Bioavailability. The available data indicate that the plasma concentrations of polyphenols and their metabolites obtained through moderate consumption of red wine, although low (of the order of 1 micromole per litre or less), are nevertheless amply sufficient to exert a beneficial action on several parameters involved in the development of cardiovascular disease. It should also be noted that there are other examples where the presence of polyphenols, even in low quantities, is associated with additional benefits on cardiovascular health. This is particularly the case for extra-virgin olive oil, whose polyphenol content is higher than regular olive oil and is considered the main factor associated with a more pronounced reduction in the risk of cardiovascular disease (see our article on this subject).
- Metabolic changes. In several clinical intervention trials, wine has been shown to be superior to other types of alcohol in favourably modulating several parameters linked to the development of cardiovascular disease. For example, randomized studies have shown that wine produces a greater improvement in insulin resistance and endothelial function than other types of alcohol, and more effectively protects vessels from oxidative stress.
For all these reasons, it has been proposed that the cardiovascular benefits of red wine could be greater than those provided by other types of alcohol, both in terms of cardiovascular health and general health.
Red wine and coronary heart disease
Although biologically plausible, the superiority of red wine on cardiovascular health remains very difficult to prove. On the one hand, it is impossible (for ethical reasons, in particular) to carry out randomized studies where we would evaluate the incidence of cardiovascular disease in a group of participants randomly assigned to consume alcoholic beverages (wine or other) regularly or not for several years. On the other hand, most moderate drinkers do not generally consume a single type of alcohol, and it therefore becomes almost impossible to distinguish the positive effect of red wine from that associated with moderate alcohol intake in general (increased HDL levels, anticoagulant activity). Nevertheless, several observations suggest that moderate consumption of red wine may represent the best way to reap the cardiovascular benefits of alcohol while minimizing its negative effects on cancer risk (discussed further, see Figure 9).
Ecological studies. A first indication of the positive effect of red wine on cardiovascular health comes from ecological studies (carried out on the scale of overall populations and not of individuals) in which the incidence of cardiovascular mortality was compared according to the average quantity of wine consumed by the inhabitants of various countries. It was noted that the countries that were the largest consumers of red wine, notably France and Italy, had a much lower incidence of mortality than those that consumed less (Figure 7). Similar results have been obtained by other groups, but although they are interesting, these ecological studies remain subject to the interference of several uncontrollable factors (cultural, socioeconomic, lifestyle-related) that can influence the results.
Figure 7. Geographic variation in cardiovascular mortality rate according to the quantity of red wine consumed.Taken from St-Leger et al. (1979).
Cohort studies. This superiority of red wine observed in ecological studies is, however, less clear in cohort studies (prospective and case-control), in which the incidence of cardiovascular disease is compared according to the type of alcohol consumed by a given group of individuals. As shown in Table 1, some studies have reported that wine drinkers were at lower risk of coronary heart disease or premature mortality than those who preferred beer or spirits, while others observed no difference between the different types of alcohol.
Table 1. Examples of studies that compared the effects of wine, beer, and spirits on the risk of coronary heart disease and mortality from various causes. *Compared to abstainers.
| Population | Alcohol consumption | Measured parameters | Change in risk* | Source |
|---|---|---|---|---|
| Superiority of wine compared to other types of alcohols | ||||
| 87,256 women | 5-15 g/day | Coronary artery disease | ↓40% (wine>beer= liquor) | Stampfer et al. (1988) |
| Stroke | ↓40% | |||
| 128,934 adults | 1-2 drinks/day | All-cause mortality | ↓20% (wine only) | Klatsky et al. (2003) |
| Coronary mortality | ↓60% (wine) | |||
| ↓30% (beer) | ||||
| 36,250 men | 22-32 g/day | All-cause mortality | ↓33% (wine only) | Renaud et al. (1992) |
| Coronary mortality | ↓45% (wine) | |||
| ↓12% (beer) | ||||
| Cancer mortality | ↓22% (wine) | |||
| ↑4% (beer) | ||||
| 24,523 adults | 8-21 drinks/week | All-cause mortality | ↓24% (wine only) | Grønbaek et al. (2000) |
| Coronary mortality | ↓36% (wine) | |||
| ↓37% (beer) | ||||
| ↓22% (liquor) | ||||
| Cancer mortality | ↓22% (wine) | |||
| ↑32% (beer) | ||||
| ↑13% (liquor) | ||||
| 1373 men | ≥ 0-20 g/week | All-cause mortality | ↓27% (wine only) | Streppel et al. (2009) |
| Coronary mortality | ↓39% (wine) | |||
| ↓18% (beer) | ||||
| ↓8% (liquor) | ||||
| 13,285 adults | 1-2 drinks/day | Cardiovascular and cerebrovascular mortality | ↓53% (wine) | Grønbaek et al. (1995) |
| ↓21% (beer) | ||||
| ↑16% (liquor) | ||||
| 513 patients | ≥ 0-4 drinks/week | Myocardial infarction | ↓60% (wine) | Rosenberg et al. (1981) |
| 918 controls | ||||
| ↓20% (beer) | ||||
| ↓10% (liquor) | ||||
| 123,840 adults | ≥2 days/week | All-cause mortality | ↓20% (wine) | Klatsky et al. (1990) |
| ↓10% (beer) | ||||
| Coronary mortality | ↓50% (wine) | |||
| ↓30% (beer) | ||||
| ↓40% (liquor) | ||||
| 2,106 men (non-smokers) | 2 drinks/day | Coronary mortality | ↓75% (wine) | Friedman et al. (1986) |
| ↓51% (beer) | ||||
| ↓34% (liquor) | ||||
| No superiority of wine compared to other types of alcohols | ||||
| 44,059 men | 2 drinks/day | Coronary artery disease | ↓2% (wine) | Rimm et al. (1991) |
| ↓20% (beer) | ||||
| ↓45% (liquor) | ||||
| 11,121 men | ≥ 1 glass/day | Coronary artery disease | ↓30% (wine) | Kozarevic et al. (1980) |
| ↓40% (beer) | ||||
| ↓20% (liquor) | ||||
| 1136 men | ≤ 48 g/day | Coronary mortality | ↓70% (wine) | Hennekens et al. (1979) |
| ↓70% (beer) | ||||
| ↓80% (liquor) | ||||
| 38,077 men | ≥ 15 g/day | Coronary artery disease | ↓52% (red wine) | Mukamal et al. (2003) |
| ↓38% (white wine) | ||||
| ↓41% (beer) | ||||
| ↓27% (liquor) |
Some studies carried out among populations who consumed alcohol mainly in the form of beer (Czech Republic, Germany or Hawaii) have found a decrease in coronary heart disease compared to abstainers, but the degree of protection offered by beer compared to that of wine remains uncertain. According to a meta-analysis, a moderate intake of beer and wine is associated in both cases with a similar reduction in the risk of cardiovascular events, while another meta-analysisshows that the protection provided by beer would be less pronounced than that observed in moderate wine drinkers. This is in agreement with a study reporting a 20% reduction in the risk of all-cause mortality and a 30% reduction in cardiovascular mortality in moderate wine drinkers compared to exclusive beer drinkers.
It is also interesting to note that the reduction in mortality risk from low amounts of alcohol seems to be very sustained among inhabitants of countries where wine is the main alcoholic beverage consumed by the population (Figure 8). For example, compared to more northern countries (England, Scandinavia), which prefer to consume alcohol in the form of beer, the reduction in mortality is more pronounced for the inhabitants of France and Italy where wine is the main drink, even at relatively high quantities of alcohol (40 g, or approximately 3 glasses per day). These data therefore suggest that while the cardiovascular benefits of red wine are similar to those of other alcoholic beverages in small quantities, the window of protection offered by red wine seems much larger than for other types of alcohol. Moreover, it is interesting to note that in the classic Seven Countries study (which established a link between cholesterol levels and the risk of cardiovascular disease), the lowest cardiovascular mortality of cohorts located in rural regions of Italy was observed in men who consumed an average of 78 g of alcohol per day (about 5 glasses), almost exclusively in the form of wine with meals. Monitoring this population for 30 years showed that this level of consumption is associated with a life expectancy 2 years higher than that of occasional drinkers or drinkers who exceeded this quantity. These observations therefore suggest that the harmful effects of alcohol are much less pronounced when this intake is in the form of red wine.
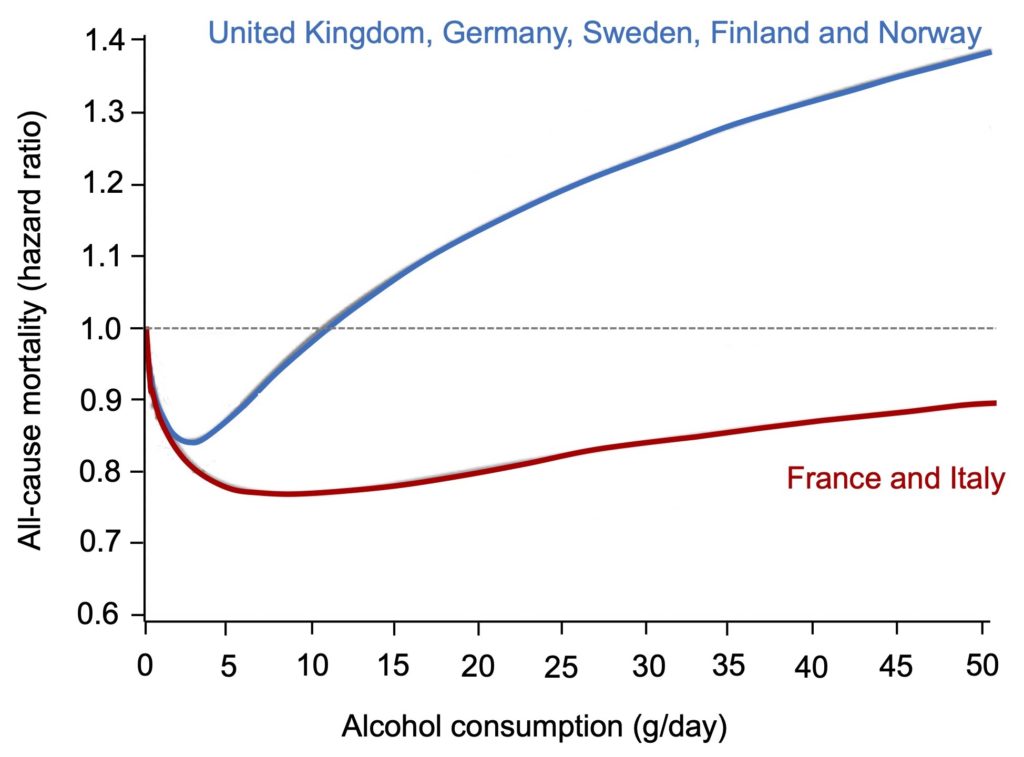
Figure 8. Comparison of the variation in the mortality rate associated with alcohol consumption between different European countries. Note the very different relationship between the amount of alcohol consumed and mortality risk for people living in France and Italy, where wine is primarily consumed, suggesting that these mortality benefits are not simply due to alcohol. Adapted from Castelnuovo et al. (2022).
Another clue to the superior effect of wine, however, more indirect in nature, comes from a part of the INTERHEART study that examined the association between alcohol consumption and the risk of myocardial infarction. In this study, it was shown that South Asia (India, Pakistan, Sri Lanka, Bangladesh) was the only region in the world where alcohol consumption was not associated with a decrease, but rather a significant increase in the risk of heart attack. It is interesting to note that the vast majority (93%) of the alcohol consumed by the inhabitants of this region is in the form of spirits, half of which is made domestically, while the consumption of wine is exceedingly rare (0.3%). It is therefore possible that alcohol consumption is more harmful to the heart when it is mainly in the form of spirits rather than red wine. Moreover, it was observed that beer and spirits drinkers had an increased risk of cardiovascular events, cirrhosis, accidents or injuries, and premature mortality compared to red wine drinkers.
Red wine and cancer
In 1988, the International Agency for Research on Cancer (IARC) classified alcohol as a group 1 carcinogen, meaning it is known to be carcinogenic to humans. It is now well established that the acetaldehyde produced during the metabolism of ethanol is a very reactive molecule, which can cause enormous damage to the genetic material of cells and thus trigger the development of cancer.
However, it seems that this carcinogenic effect is less pronounced for red wine than for other types of alcohol. For example, a Danish study showed that drinking 8-21 glasses of wine per week was associated with a 22% reduction in cancer mortality, while conversely the same amount of alcohol in the form of beer or spirits increases the risk of mortality linked to this disease by approximately 20%. This difference is probably due to the very different effect of these types of alcohol on the risk of cancer of the upper digestive system (mouth, pharynx, esophagus), organs particularly vulnerable to the carcinogenic effects of alcohol: while consumption of beer or spirits (7-21 glasses per week) increases the risk of these cancers by 300%, the same amount of alcohol in the form of wine reduces this risk by 50%. This difference between wine and other types of alcohol is also observed for several other types of cancers. For example, one study showed that while beer and spirits drinkers are at greater risk of lung cancer, moderate consumption of red wine is associated with a significant reduction in the risk of this cancer. A Montreal study reported that the increase in the risk of several types of cancer associated with alcohol consumption is restricted to beer and spirits drinkers and is not observed among wine drinkers, with even a substantial reduction in the risk of certain types of cancers (esophagus, liver, pancreas, and colon, in particular) (Figure 9).
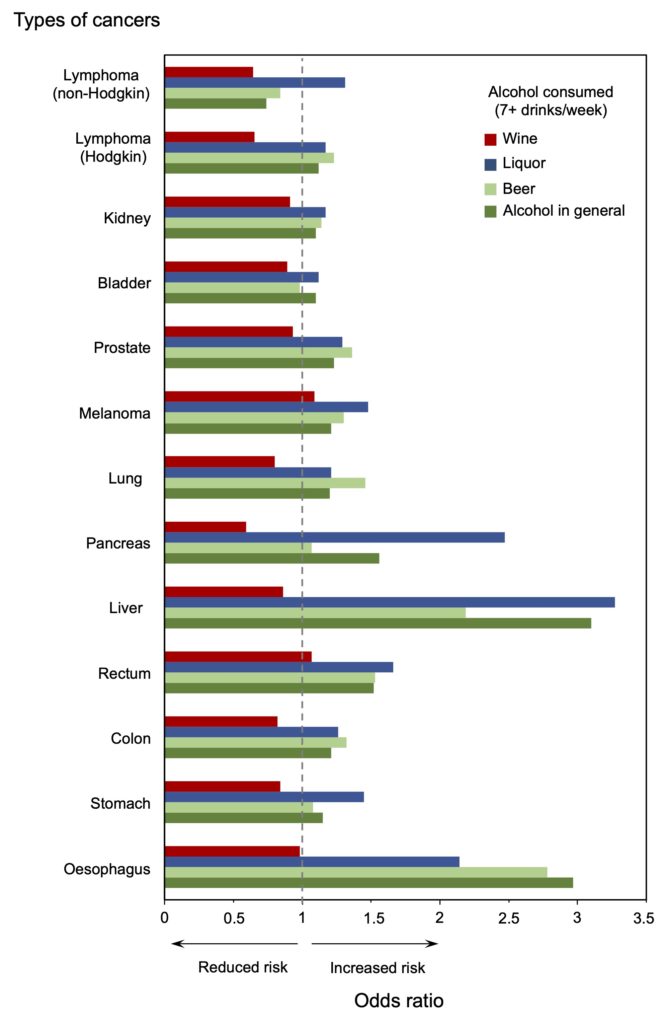
Figure 9. Relationship between the type of alcohol consumed and the risk of different cancers. Risks were calculated using abstainers as the reference group. Note that for all of these cancers, the increase in risk associated with alcohol consumption is much lower among wine drinkers (red rectangles). From Benedetti et al. (2009).
A difference between wine and other types of alcohol on the risk of cancer is also suggested by a large-scale study, carried out among a million women followed for 10 years, which showed that the increase in the risk of liver, mouth and colon cancer affecting beer and spirits drinkers disappears almost completely in those who prefer wine, and is even associated with a reduced risk in the case of colon cancer. A lower risk of cancer associated with drinking wine rather than other types of alcohol has also been observed in other studies for liver, pancreatic, prostate and ovarian cancers. Recently, an analysis of 73 studies detected no association between red wine consumption and the risk of several digestive, gynecological or other cancers (kidney, skin, lung, brain).
Since ethanol in wine is metabolized to acetaldehyde in a similar manner to that of other types of alcohol, it has been proposed that the antioxidant and anti-inflammatory properties of phenolic compounds in red wine could mitigate the negative effects of this toxic molecule and at the same time reduce the risk of cancer. Resveratrol has received considerable attention in this regard, because this molecule interferes with a large number of processes involved in the development of cancer. Although resveratrol is metabolized very rapidly following absorption, it has been observed that its metabolites (resveratrol sulfates) are taken up by cells and retain their biological activity, suggesting that resveratrol concentrations achieved by moderate consumption of red wine would be sufficient to induce cell growth arrest.
Overall, these observations suggest that the risk of developing certain cancers linked to alcohol consumption is generally lower among wine drinkers than among those who drink other types of alcohol. This obviously does not mean that wine consumption is without risk (the increased risk of breast cancer associated with moderate consumption of all types of alcohol, including red wine, is a reminder of this reality), especially if it exceeds the recommended thresholds of 1 drink per day for women and 2 drinks per day for men. However, for people who regularly drink alcohol, there is little doubt that a moderate intake of red wine represents the best choice to reap the benefits of alcohol in reducing the risk of coronary heart disease while minimizing its negative effects on cancer risk. This superiority of red wine is well illustrated by the absence of a significant increase in the risk of mortality among wine drinkers, even at fairly large quantities of alcohol, compared to the significant increase observed among beer and spirits drinkers. (Figure 10).
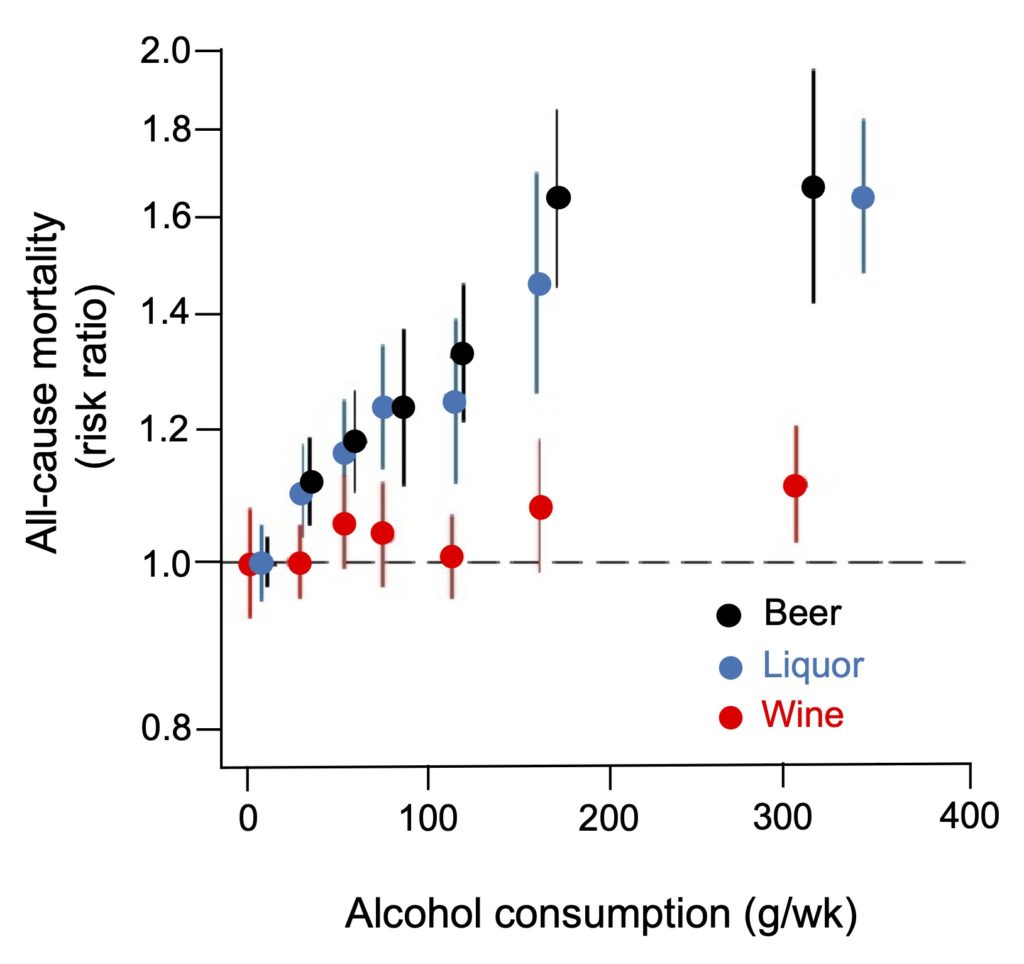
Figure 10. Comparison of increases in mortality risk associated with the consumption of different types of alcoholic beverages. As mentioned in the legend to Figure 3, mortality risks are established using light drinkers as the reference group, which eliminates the benefits usually observed for low amounts of alcohol. However, the data clearly shows that for an equivalent quantity of alcohol, the risk of mortality is much lower among wine consumers. From Wood et al. (2018).
Ideal consumption pattern
To get the most benefits out of moderate amounts of alcohol, one can take inspiration from the Mediterranean diet, in which alcohol is consumed moderately during meals, usually in the form of wine. A very large number of studies have shown that this dietary pattern is associated with a significant reduction in the risk of cardiovascular disease, and it has been suggested that moderate wine consumption alone is responsible for 25% of these benefits, which is as much as the high fruit and vegetable intake characteristic of this diet. At the metabolic level, this important contribution of alcohol is possibly linked to its positive effect on the control of blood sugar and inflammation, but its psychosocial impact should not be overlooked, particularly on the reduction of chronic stress. Another advantage of this drinking pattern is that moderate alcohol intake is spread out over the week, thereby minimizing binge-drinking episodes, where high alcohol intake in a short period of time drastically increases the risk of health problems, including cardiovascular ones. It is well established (see here and here, for example) that for the same quantity of alcohol, the reduction in the risk of myocardial infarction is much more marked for people who drink small quantities regularly (≥ 2 days or more per week) than for those who consume this quantity on 1 or 2 occasions. Consumption spread over several days per week results in a significant reduction in the risk of mortality (Figure 11), and it is likely that this benefit is even greater if the alcohol consumed is mainly in the form of red wine.
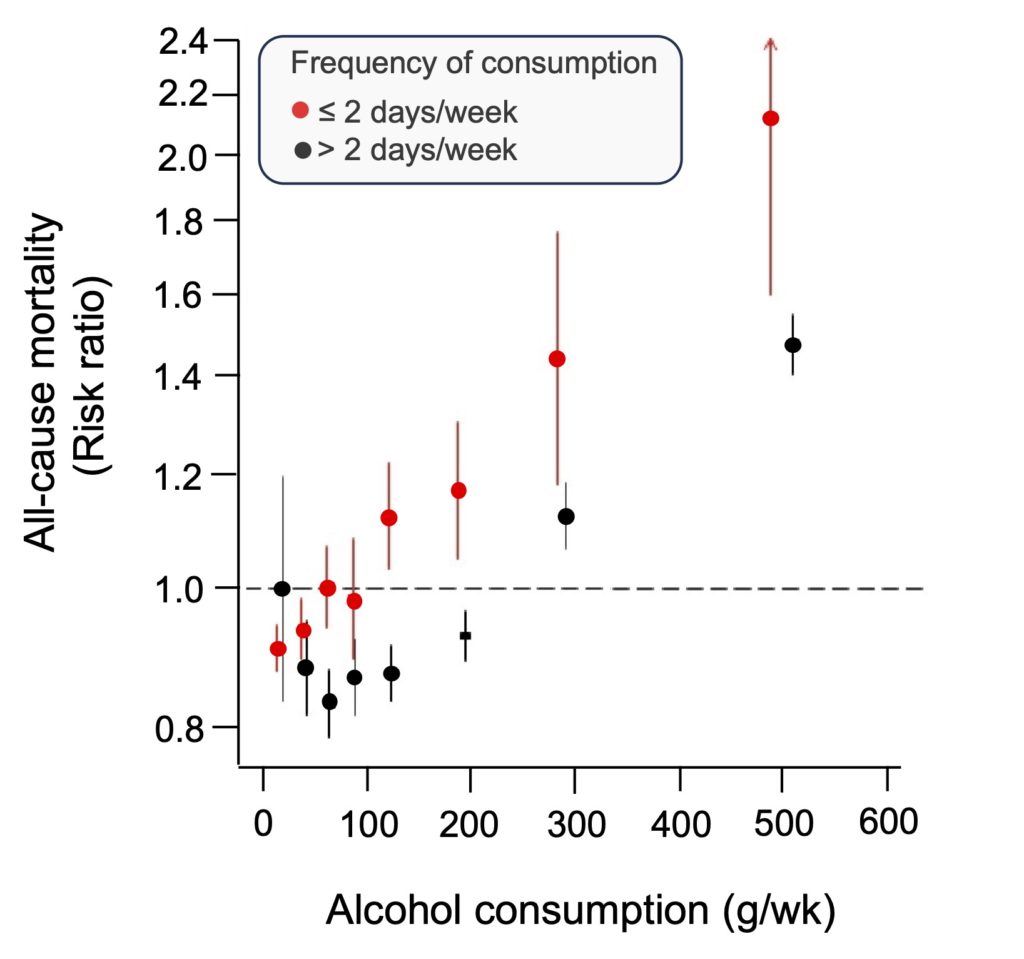
Figure 11. Variation in mortality risk according to frequency of alcohol consumption. Note the reduction in mortality risk for alcohol consumption (all types combined) of up to 200 g per week (approximately 14 drinks) when the quantity of alcohol is spread over several days of the week. From Wood et al. (2018).