Dr Éric Thorin, Ph. D.
Professeur titulaire, Département de Chirurgie, Université de Montréal. Chercheur au centre de recherche de l'Institut de cardiologie de Montréal.
See all articlesOverview
- In all mammals, there is a strong correlation between resting heart rate and average lifespan within a species.
- In humans, a high resting heart rate (>100 beats per minute) promotes chronic inflammation, heart disease, electrical (rhythmic) disturbances of the heart, hypertension, atherosclerosis, and obesity.
- The mechanical strain imposed by the cycles of cardiac contractions damages arteries over time and compromises the integrity of large blood vessels.
- The good news is that regular physical activity slows the resting heart rate and prolongs healthy life expectancy.
Connected devices are now part of our daily lives, and many people wear a watch that continuously monitors their heart rate. This is a useful parameter for doctors and for people exercising who want to reach target heart rates or avoid exceeding a certain threshold, such as participants in a cardiac rehabilitation program. But what does this parameter mean? What is its physiological and potentially pathological significance? How is it regulated? Here are some answers.
Resting heart rate (RHR) is associated with longevity.
The average RHR value influences our healthy life expectancy. This relationship holds true for all wild mammals (Fig. 1), with one exception today: as Figure 1 shows, humans have deviated from this relationship, beginning a little over 250 years ago. Life expectancy for our species (approximately 30 years in the mid-18thcentury) began to increase slightly at the beginning of the 19th century due public health efforts (sewers, drinking water). It then accelerated sharply from the end of the 19th century with the systematization of vaccination, validated by Pasteur in 1885; by 1950, human life expectancy at birth had more than doubled! Advances in medicine in the early 1960s, a period often referred to as the cardiovascular revolution, then allowed it to increase by a further 12% until the beginning of this century.
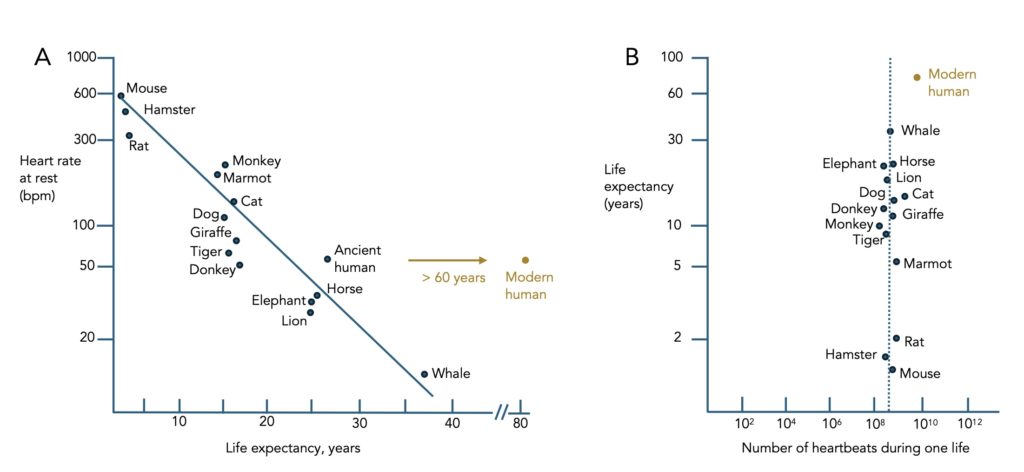
The reason heart rate (HR) is so strongly associated with longevity is that it is an important physiological parameter. It is represented by the number of heartbeats per minute (bpm) under normal resting conditions: it ranges between 60 and 95 bpm during the day and between 40 and 60 bpm during sleep. Early physicians in antiquity, such as the Greek physician Claudius Galen (2nd century AD), could predict the health of their patients based on their HR, and even today, an abnormally high HR—the threshold for tachycardia is set at 100 bpm at rest—is often indicative of high blood pressure (hypertension), being overweight, reduced lung function, and a lower level of physical activity. There is also a correlation between FCR and markers of inflammation (C-reactive protein and fibrinogen) and a predominance of activity of the sympathetic nervous system, whose neurotransmitters are adrenaline and noradrenaline.
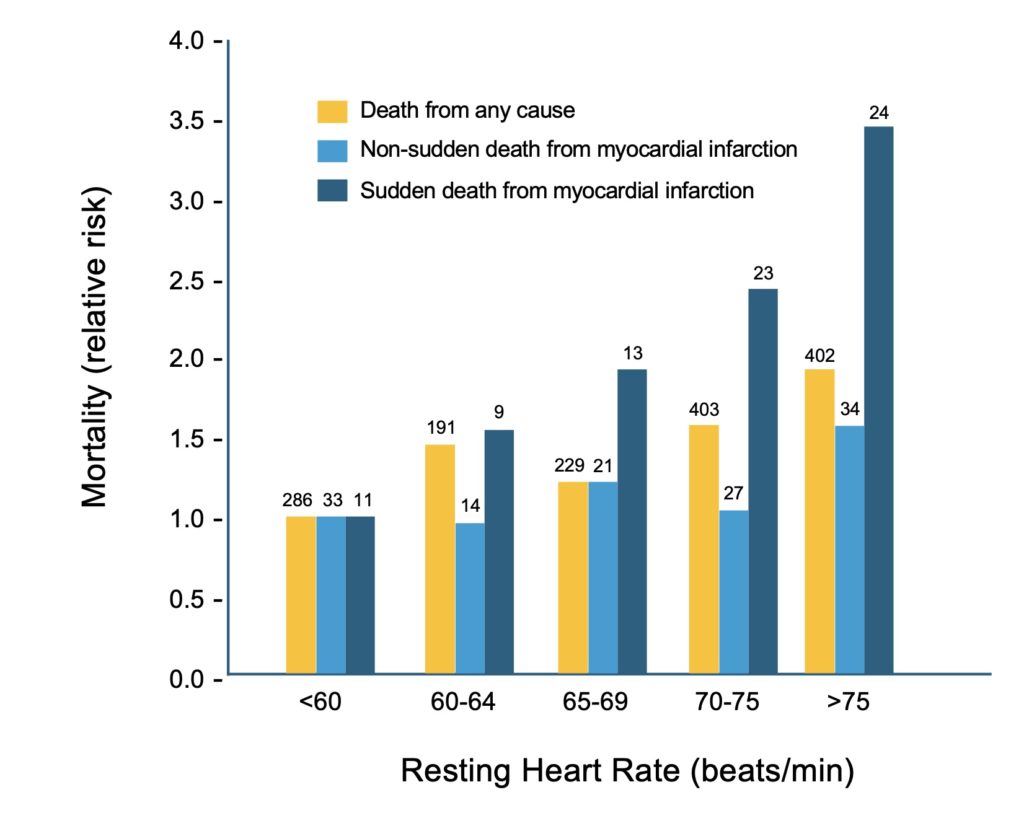
Despite the increase in our life expectancy, the link between FCR and life expectancy is maintained. For example, the Paris study carried out by the team of Dr Xavier Jouven established a direct link between a high FCR and an increased risk of mortality, particularly cardiovascular, in middle-aged men (Fig. 2). By following 4,320 men over 20 years, analyses revealed that an increase in FCR increases the risk of premature mortality by 47% over time, while a decrease in FCR reduces it by 18 %.
How can we explain this close relationship between heart rate and longevity?
The heart’s role is to create a constant blood flow to meet the energy needs of the organs (oxygen, nutrients), as well as to transport various elements essential to their function (e.g., hormones, immune cells, stem cells). Cardiac output—defined as the volume of blood ejected into the aorta by the left ventricle with each heartbeat—is therefore the determining parameter of this function, since cardiac output varies according to the organs’ energy needs; for example, heart rate will increase after a meal to increase blood flow to the intestines (due to digestion) or, during physical activity to fuel the muscles.
Yet movement involves a degree of mechanical stress, and therefore inevitably wear and tear, especially on the blood vessels. To create a constant flow of blood, pressure must be generated and maintained, and the heart alone is not enough; it must work together with the aorta, the artery that originates at the base of the left ventricle of the heart and forms the common trunk of the arterial system. It is common knowledge that the heart acts as a muscular pump, ejecting oxygenated blood towards the aorta during systole (the cardiac contraction phase). It is less well known that due to its elasticity, the aorta acts as a second pump, first by relaxing during systole to cushion the sharp increase in blood pressure and store blood (Fig. 3A), then by returning to its original shape during diastole (the heart’s relaxation phase) to propel blood to the periphery while maintaining blood pressure (Fig. 3B).
This is the Windkessel effect (German for “air chamber”). This ventriculo-aortic coupling ensures the efficient distribution of blood throughout the body. Good aortic health (elasticity) is therefore as important as the strength of the heart for effective blood circulation. In addition to maintaining a constant blood flow, the high pressure created by cardiac ejection is dampened by the elasticity of the aorta and kept at approximately 120 millimetres of mercury (mmHg). When the heart relaxes (diastole), the return of the aorta to its original size also prevents a drop in perfusion pressure by maintaining it at approximately 80 mmHg. Ultimately, the aorta and its two large immediate branches (the carotid arteries) dampen the pulsatility of blood flow. By reducing the pulsation force, its immediate branches, the arteries, which are more muscular than elastic, can take over. When blood leaves the small (purely muscular) arterioles of the organs, its flow is weak, almost non-pulsatile, with a very low pressure of approximately 10 to 5 mmHg. The blood thus enters the capillaries, the site of all exchanges between the blood and the organs, without damaging them. Imagine an ossified aorta (a copper pipe): the flow and pressure would be equivalent to those created by opening and closing a running water tap 70 times per minute! The aorta is therefore crucial for maintaining blood flow. But it undergoes this mechanical stress approximately 100,000 times a day!
What are the consequences of pulsatile blood pressure and flow on blood vessels?
Consequently, over time, the aorta will wear down and stiffen (like a rubber tube). The consequence of this stiffening, and therefore the loss of elasticity (also called loss of compliance), is isolated systolic hypertension, a condition defined by an increase in pressure during systole (> 140 mmHg) without a change in diastolic pressure (< 90 mmHg). This condition generally develops later in life than hypertension, and the use of low doses of antihypertensive medications has protective effects against stroke, myocardial infarction, and heart failure.
In the vascular system, however, the weakest link by far is coronary circulation, as these arteries are the most exposed to the mechanical stress of each heartbeat. The coronary arteries are the first branches of the aorta; they are more muscular than elastic and run along the epicardium (the surface of the heart muscle, called the myocardium). Their branches, the muscular arterioles, penetrate directly into the myocardium, which is only 1 cm thick. They branch out, perfuse, and nourish the entire heart muscle. However, during systole (contraction of the heart muscle), the arterioles are compressed by the force of contraction of the heart muscle, and blood flow is interrupted. Thus, the heart muscle, the very muscle that initiates blood flow, is only perfused during diastole, its resting phase. It is, therefore, due to the elastic recoil of the aorta and the resulting propulsive effect (Fig. 3B) that blood flows into the coronary arteries. No other arteries in the human body undergo such mechanical stress, and therefore these are the ones that wear out the fastest. The damage begins early, in one’s twenties, evidenced by the appearance of small, benign fatty plaques inside the epicardial coronary arteries. Over time (measured in decades, but always accelerated by risk factors such as a sedentary lifestyle, hypertension, diabetes, and dyslipidemia) and the repeated wear and tear with each heartbeat, these plaques will enlarge, calcify, and eventually narrow these large arteries. This can manifest as angina pectoris, or angina pain during exertion, due to the reduced capacity of the myocardium to increase blood flow, as it requires more oxygen, thus causing damage to the muscle cells. Ultimately, the plaque can rupture, which immediately activates platelets and creates a blood clot that obstructs the artery and causes a myocardial infarction (heart attack); this is the leading cause of death in both women and men in high-income countries like Canada. It’s no wonder, then, that these are the arteries that most often require repair during our lives when angina pain becomes debilitating, either through bypass surgery or angioplasty with the placement of a stent to open the blocked coronary artery and keep it open.
How can we maintain optimal heart rate variability (HRV) to reduce biomechanical stress and delay vascular damage?
Unsurprisingly, the best way to achieve this is through regular exercise. The sympathetic nervous system (adrenaline, noradrenaline) drives the heart rate upward and the parasympathetic nervous system (acetylcholine) slows it down. Regular exercise increases the influence of the parasympathetic system, leading to a new equilibrium that favours a lower resting heart rate (RHR). Professional athletes in endurance sports like cycling have RHRs as low as 30 bpm—which can have detrimental effects on the heart rhythm (the electrical signal)—but the optimal heart rate range is between 50 and 85 bpm.
A second, less well-known benefit is that acetylcholine, released by the nerve endings of the parasympathetic nervous system, has a direct anti-inflammatory effect. Consequently, when the influence of the parasympathetic system is weak (as is the case in physically inactive individuals), the sympathetic system predominates, thereby promoting a higher RHR and lower baseline inflammation. Over time, this imbalance will not only promote the formation of plaques in the coronary arteries, but also decrease the elasticity of the aorta and carotid arteries, contributing to isolated systolic hypertension.
There is a third, well-known effect of exercise that is independent of the nervous system: when heart activity increases due to physical activity, the transient increase in blood flow in the vessels mechanically stimulates the endothelium, the layer of cells lining the lumen of the arteries. This variation in frictional forces on the endothelium has a protective effect by releasing nitric oxide (pharmacologically mimicked by nitroglycerin, a widely used antianginal drug) which prevents or slows the formation of the first benign fatty plaques and helps to reduce existing plaques, even in patients with coronary artery disease.
In short, it is undeniable and undisputed that the higher the heart rate, the greater the risk of cardiovascular disease and premature death. More than just an assessment of the number of heartbeats, heart rate variability (HRV) is actually a concrete measure of the body’s health, reflecting the concerted action of numerous physiological mechanisms, both positive and negative, that interact to maintain the body’s equilibrium. Regular exercise is absolutely essential to ensure proper control of these mechanisms and remains the only known way to date to maintain optimal HRV without medication.