Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesUpdated June 8, 2020
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the SARS-CoV-2 coronavirus strain that primarily, but not exclusively, affects the respiratory system. While in the majority of infected people the symptoms of the disease are relatively mild or moderate (cough, fever, dyspnea or difficulty breathing, digestive disorders, temporary loss of taste and smell, hives, vascular lesions on the fingertips and toes), they may worsen in some people who have one or more risk factors (diabetes, hypertension, obesity, cardiovascular disease, advanced age) into acute respiratory distress syndrome that requires hospitalization in an intensive care unit and can lead to death.
There is no vaccine or effective drug available to reduce the mortality associated with COVID-19. The use of an antiviral drug, remdesivir, which was urgently approved by the FDA on May 1, 2020, reduces the number of days in hospital in people with COVID-19, but does not significantly reduce mortality. As of May 15, 2020, more than 1,500 studies on various aspects of COVID-19 have been registered on ClinicalTrials.gov, including more than 885 intervention studies and randomized controlled studies, with 176 on the use of hydroxychloroquine.
Hydroxychloroquine
One of the first candidates tested for treating COVID-19 was hydroxychloroquine, a drug used for its anti-inflammatory properties in the treatment of rheumatoid arthritis and systemic lupus erythematosus. Prior to the current COVID-19 pandemic, it was already known that chloroquine and its derivatives, including hydroxychloroquine, have non-specific antiviral activity against several types of enveloped viruses (HIV, hepatitis C, dengue, influenza, Ebola, SARS, MERS) in vitro. Two recent studies (see here and here) have shown that hydroxychloroquine also inhibits infection with the SARS-CoV-2 virus in vitro, i.e. in cultured epithelial cells. Hydroxychloroquine, which has a better safety profile than chloroquine, has been shown to be a more potent SARS-CoV-2 inhibitor in vitro.
The results obtained in vitro do not necessarily imply that chloroquine and its derivatives have antiviral activity in humans. Indeed, studies have shown that in vivo chloroquine and/or hydroxychloroquine have no effect on viral replication or increase viral replication and the severity of illness caused by infection by influenza, dengue, Simliki forest virus, encephalomyocarditis virus, Nipah and Hendra viruses, Chikungunya virus, and Ebola virus (references here).
Initial results from studies on the use of hydroxychloroquine to treat COVID-19 are unclear. Chinese researchers have reported treating over 100 patients with beneficial effects, but have not released any data. French microbiologist Didier Raoult and his collaborators published two articles (see here and here) on the use of hydroxychloroquine (in combination with the antibiotic azithromycin) for the treatment of COVID-19, in which they concluded that this drug lowers viral load in nasal swabs. However, these studies were not randomized and they do not report essential clinical data, such as the number of deaths among participants. In addition, two other French groups (see here and here) report having found no evidence of antiviral activity of hydroxychloroquine/azithromycin or of clinical benefit in hospitalized patients with a severe form of COVID-19.
In an observational study conducted in New York City hospitals, hydroxychloroquine was administered to 811 patients out of a total of 1376 patients, with a follow-up lasting an average of 22.5 days after admission to the hospital. Analysis of the results indicates that among this large number of patients admitted to hospital with a severe form of COVID-19, the risk of having to be intubated or dying was not significantly higher or lower in patients who received hydroxychloroquine than in those who did not. The authors conclude that the results obtained do not support the use of hydroxychloroquine in the current context, except in randomized controlled trials, which remain the best way to establish the efficacy of a therapeutic intervention.
Cardiovascular risk: Prolongation of the QT interval
Although hydroxychloroquine and azithromycin are well-tolerated drugs, both can cause prolongation of the QT segment on the electrocardiogram (figure below). For this reason, cardiologists are concerned about the use of these two drugs in a growing number of clinical trials for the treatment of COVID-19 (see here, here, here and here). It should be noted that the prolongation of the corrected QT interval (QTc) is a recognized marker of an increased risk of fatal arrhythmias.
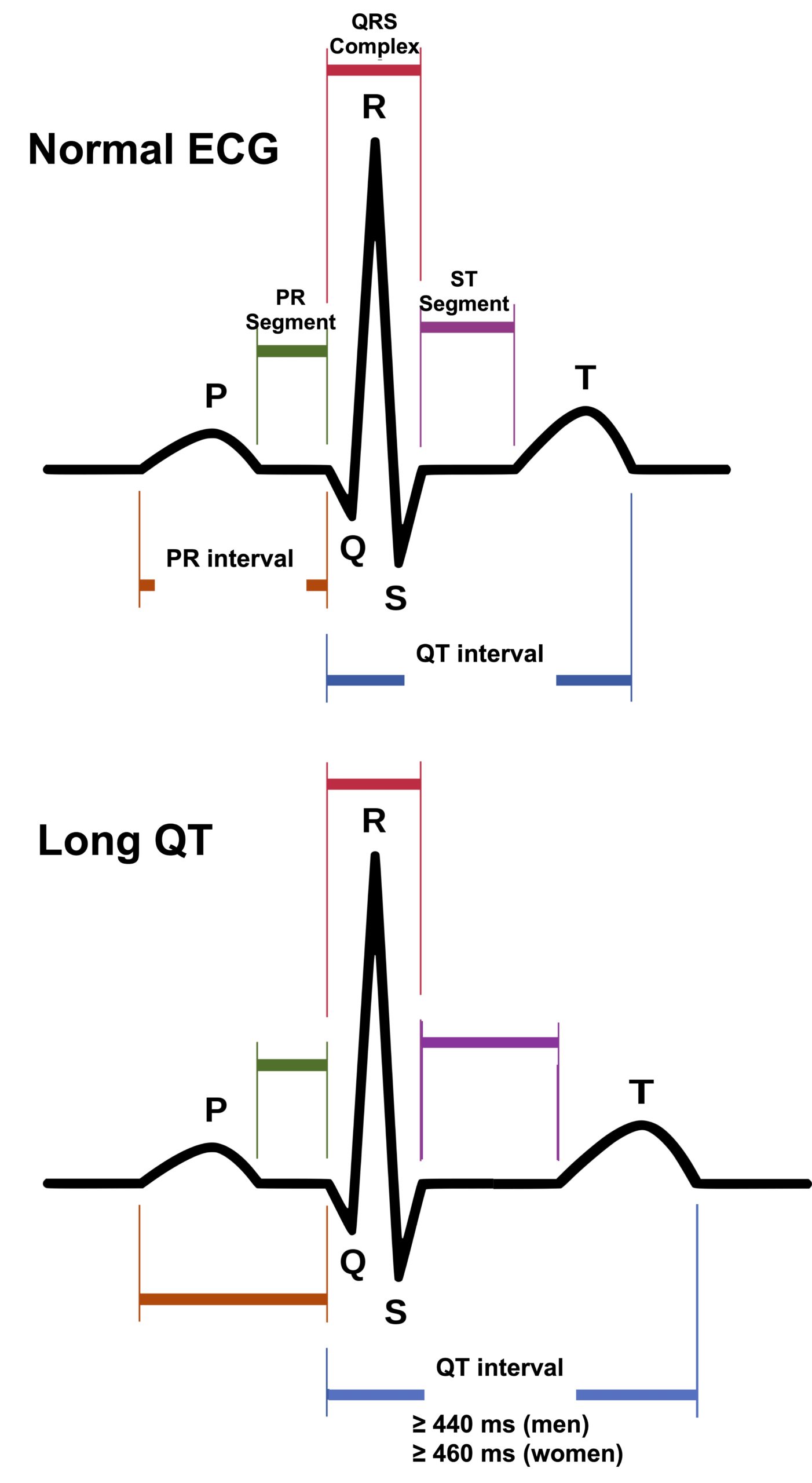
Figure. Normal and abnormal (long) QT interval on the electrocardiogram.
Hospital researchers in the United States assessed the risk of QTc prolongation in 90 patients who received hydroxychloroquine, 53 of whom were concomitantly given the antibiotic azithromycin. The most common comorbidities among these patients were hypertension (53%) and type 2 diabetes (29%). The use of hydroxychloroquine alone or in combination with azithromycin was associated with QTc prolongation. Patients who received the two drugs in combination had significantly greater QTc prolongation than those who received hydroxychloroquine alone. Seven patients (19%) who received hydroxychloroquine monotherapy saw their QTc increase to 500 milliseconds (ms) or more, and three patients (8%) saw their QTc increase by 60 ms or more. Among the patients who received hydroxychloroquine and azithromycin in combination, 11 (21%) saw their QTc increase to 500 milliseconds (ms) or more, and 7 (13%) saw their QTc increase by 60 ms or more. Treatment with hydroxychloroquine had to be stopped promptly in 10 patients, due to iatrogenic drug events (adverse reactions), including nausea, hypoglycemia and 1 case of torsades de pointes. The authors conclude that physicians treating their patients with COVID-19 should carefully weigh the risks and benefits of treatment with hydroxychloroquine and azithromycin, and monitor QTc closely if patients are receiving these drugs.
French doctors have also published the results of a study on the effects of hydroxychloroquine treatment on the QT interval in 40 patients with COVID-19. Eighteen patients were treated with hydroxychloroquine (HCQ) and 22 received hydroxychloroquine in combination with the antibiotic azithromycin (AZM). An increase in the QTc interval was observed in 37 patients (93%) after treatment with antiviral therapy (HCQ alone or HCQ + AZM). QTc prolongation was observed in 14 patients (36%), including 7 with a QTc ≥ 500 milliseconds, 2 to 5 days after the start of antiviral therapy. Of these 7 patients, 6 had been treated with HCQ + AZM and one patient with hydroxychloroquine only, a significant difference. The authors conclude that treatment with hydroxychloroquine, particularly in combination with azithromycin, is of concern and should not be generalized when patients with COVID-19 cannot be adequately monitored (continuous monitoring of the QTc interval, daily electrocardiogram, laboratory tests).
Update June 8, 2020
A randomized, placebo-controlled study suggests that hydroxychloroquine is not effective in preventing the development of COVID-19 in people who have been exposed to the SARS-CoV-2 virus. The study, conducted in the United States and Canada, was published in the New England Journal of Medicine. Of 821 participants, 107 developed COVID-19 during the 14-day follow-up. Among people who received hydroxychloroquine less than four days after being exposed, 11.8% developed the disease compared to 14.3% in the group who received the placebo, a non-significant difference (P = 0.35). Side effects (nausea, abdominal discomfort) were more common in participants who received hydroxychloroquine than in those who received a placebo (40% vs. 17%), but no serious side effects, including cardiac arrhythmia, were reported. Clinical trials are underway to verify whether hydroxychloroquine can be effective in pre-exposure prophylaxis.