Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesOverview
- Excess weight, particularly when present in the abdominal area, is an important risk factor for cardiovascular disease and premature mortality.
- A new class of drugs, incretin agonists such as semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound), can achieve substantial weight loss, up to 15 to 20% of initial body weight.
- Two recent studies report that these weight losses are associated with a spectacular improvement in the clinical status of heart failure patients and a reduction in the risk of cardiovascular events in high-risk patients.
The incidence of obesity has increased dramatically in recent decades, with an estimated 600 million adults and 100 million children now obese worldwide. This is a very worrying trend, as it has been clearly established that excess weight, and particularly obesity, is a major cause of several chronic diseases and premature mortality. For example, a large study of nearly 4 million people showed that a body mass index (BMI) higher than normal (20-25) is associated with a significant increase in the risk of dying prematurely (Figure 1). This association is particularly evident for obese people (BMI>30) and especially very obese people (BMI>35), but it is also significant for overweight people (BMI between 25-30).
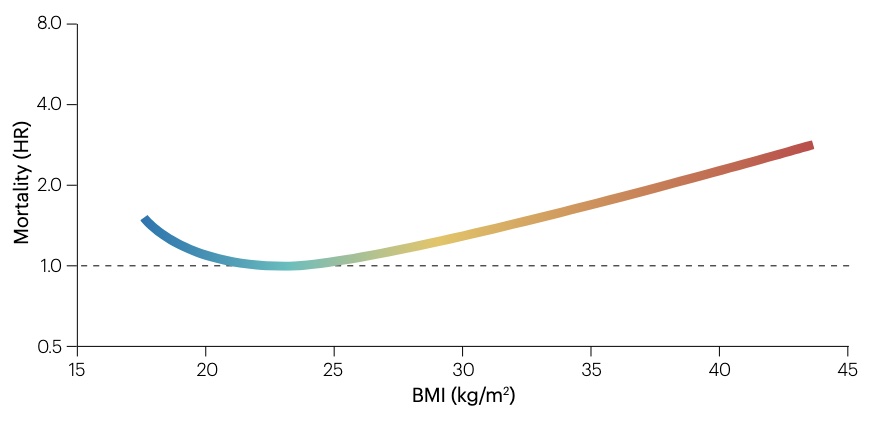
Figure 1. Relationship between body mass index and mortality risk. Data come from 189 studies (n = 3,951,455 people living in 32 countries around the world, spread across 4 continents). Adapted from Valenzuela et al. (2023).
Cardiovascular disease is a good example of this negative effect of excess weight on health. It is estimated that of the 4 million deaths caused by excess weight in 2015, more than two thirds were directly linked to cardiovascular disease due to the disastrous effect of obesity on several risk factors (type 2 diabetes, hypertension, hyperlipidemia) that considerably increase the risk of heart attack, stroke and heart failure.
For example, a meta-analysis of about twenty studies involving more than 300,000 people showed that each increase of 5 units in BMI was associated with a 30% increase in the risk of ischemic diseases (heart attacks, in particular). About half of this increase is thought to be caused by the effect of excess weight on blood pressure and blood cholesterol levels, while the other half is thought to be due to excess fat itself.
Visceral fat
Several studies indicate that it is mainly fat accumulated in visceral adipose tissue (VAT) that is associated with an increased risk of cardiometabolic diseases (Figure 2). This excess of visceral fat comes largely from the saturation of subcutaneous adipose tissue (SAT), which is normally responsible for managing energy reserves. When the adipocytes of the SAT are no longer able to increase sufficiently in number and size to store excess fat, it is then redirected towards the VAT, mainly in the abdomen (liver, pancreas) as well as in the heart (Figure 2).
It is now well documented that abnormal fatty deposits in the liver (non-alcoholic fatty liver disease) are strongly correlated with the presence of metabolic syndrome, a constellation of risk factors associated with an increased risk of type 2 diabetes and of cardiovascular disease. Recent data indicate that excess visceral fat around the heart, particularly in the structure covering the myocardium (the epicardium), could also contribute to this increased risk of cardiometabolic diseases. This fat deposit is in close contact with the heart muscle and the coronary arteries that feed it, and this proximity makes the heart particularly vulnerable to metabolic upheavals caused by excess fat. It has also been observed that the volume of epicardial fat is closely correlated with the degree of obesity and is associated with the risk of cardiovascular events.
The mechanisms responsible for the negative effect of these fat deposits on the VAT of the liver and heart are very complex (Figure 2), but simply put, the presence of this excess fat is interpreted as an “aggression” by the immune system and causes the development of a pro-inflammatory climate, both locally and throughout the body, which reduces the effectiveness of the insulin response. The combination of these two conditions (chronic inflammation and insulin resistance) represents an important risk factor for cardiovascular disease and would therefore contribute to the increase in cardiovascular events and premature mortality observed in obese people in epidemiological studies.
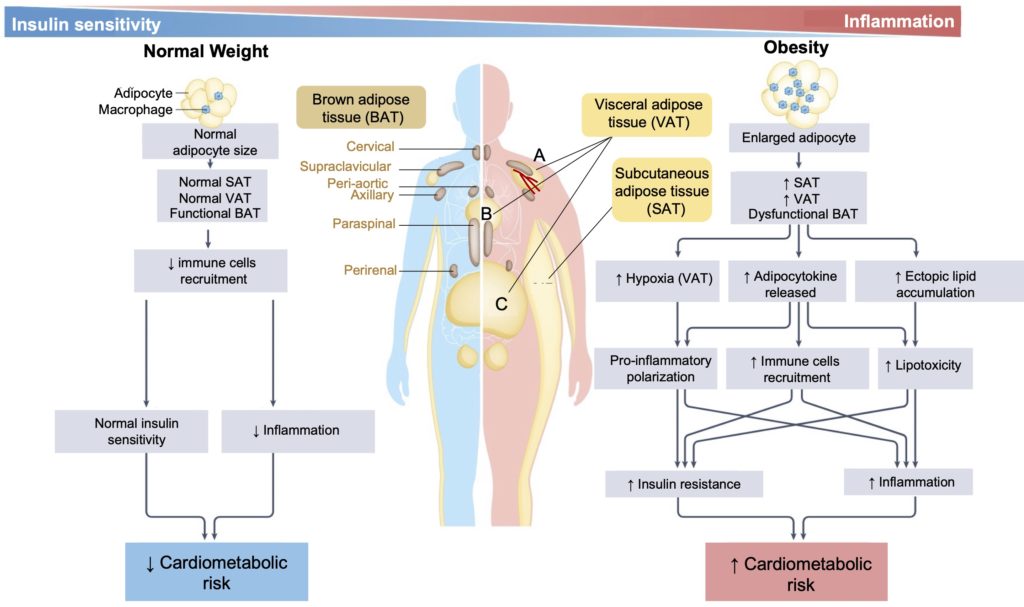
Figure 2. Main mechanisms involved in the increased risk of cardiometabolic diseases in overweight people. In the human body, fat reserves are stored in three distinct types of adipose tissue, each of which is modified during the development of obesity (right portion of the figure). Hypertrophy of adipocytes in subcutaneous adipose tissue (SAT) allows significant accumulation of fat in the periphery of the body, but when the quantity of excess fat exceeds a certain limit, fat begins to accumulate in visceral adipose tissue (VAT), around blood vessels (perivascular) (A), heart (B), and abdomen (C). Obesity also appears to disrupt the function of brown adipose tissue (BAT), a specific type of fat that is specialized for heat production, but the effects of this disruption remain poorly understood. However, we do know that it is the ectopic accumulation of fats in the VAT that is mainly responsible for the cardiometabolic problems associated with obesity. At the organ level, excess fat is toxic (lipotoxicity) and leads to recruitment of immune cells which, collectively, create pathophysiological conditions leading to the development of insulin resistance and the establishment of chronic inflammatory conditions, two important risk factors for cardiovascular disease. Adapted from Valenzuela et al. (2023).
Weight loss
The negative effect of excess weight, especially when localized at the visceral level, suggests that in obese people, body weight loss should in principle reduce the risk of cardiometabolic diseases. Studies suggest that this is indeed the case, but that the weight loss required to counteract the long-term negative effects of obesity on the cardiovascular system must be substantial. For example, one of the largest clinical trials of lifestyle modification for the treatment of obesity (Look AHEAD) failed to show a significant reduction in cardiovascular events or mortality after a 10-year follow-up. This lack of effect is probably due to the relatively low weight loss (around 6%) achieved by the majority of participants. This is in line with several intervention trials showing that although weight loss typically achieved through lifestyle interventions (5-10 kg) improves certain cardiovascular disease risk factors (systemic inflammation, endothelial dysfunction, metabolic syndrome parameters), there is no major reduction in the risk of cardiovascular disease. However, a subsequent analysis of the Look AHEAD study showed that participants who had lost ≥10% of their body weight had a significant reduction in cardiovascular events. The importance of substantial weight loss in achieving a significant reduction in the risk of cardiovascular events is also suggested by studies investigating the effects of bariatric surgery, an invasive procedure where weight losses of 10 to 40 kg are typically observed. For example, a Swedish study reported significantly lower rates of fatal and non-fatal cardiovascular events in patients who underwent this surgery.
Anti-obesity drugs
As we mentioned in a previous article, one class of drugs is currently receiving a lot of attention for its unprecedented effects on weight loss. These drugs, in particular semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound), are single or double agonists (activators) of certain receptors involved in the control of blood glucose levels, and it is for this reason that they were initially developed for the treatment of type II diabetes. However, clinical trials have shown that these drugs cause very significant weight loss in obese patients, very often greater than 15% of their initial body weight, even in the absence of diabetes (Figure 3). These drugs therefore offer a unique opportunity to examine the impact of weight loss on the risk of cardiovascular disease.
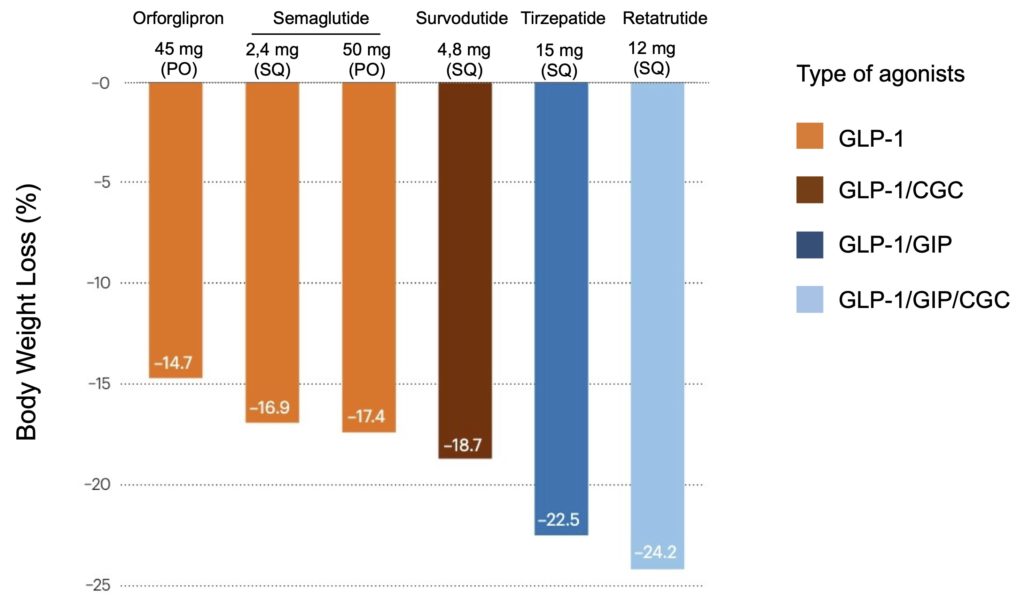
Figure 3. Comparison of body weight losses achieved following treatment with new generation anti-obesity drugs. Note that semaglutide (Wegovy) and tirzepatide (Zepbound) are currently the only agents approved by regulatory agencies for weight loss. Orforglipon, survodutide, and retatrutide are still in Phase 2/3 clinical trials. These drugs are either pure GLP-1 receptor agonists (activators) (orange), dual agonists of GLP-1 and CGC (glucagon) (red) or GLP-1 and GIP (dark blue), or triple agonists of GLP-1, GIP and GCG (pale blue). N.B.: PO; per os (orally, every day), SQ: subcutaneous (by injection, once a week).
Heart failure
It is in this context that two recent studies on one of these new molecules (semaglutide) have particularly attracted the attention of the medical and scientific communities. The first study investigated the effect of treatment with semaglutide on symptoms associated with heart failure, a serious and incurable disease that affects more than 64 million people worldwide and is a major cause of mortality and deterioration in quality of life (see box).
A heart out of breath
In heart failure, the heart does not pump enough blood to meet the body’s oxygen needs, leading to fatigue, difficulty breathing, and great difficulty (or inability) to perform simple tasks such as climbing a few steps or carrying grocery bags. This loss of efficiency of the heart muscle can be caused by direct damage to its structure, for example following a heart attack, or indirectly, following prolonged exposure to excessively high blood pressure: to compensate for the greater resistance blood vessels and allow the blood to circulate, the heart muscle has to increase its workload and over time becomes thicker and stiffer.
Clinically, this dysfunction of the heart is analyzed by measuring the ejection fraction, i.e., the quantity of blood that the left ventricle pumps with each contraction. For example, an ejection fraction of 60% means that 60% of the total amount of blood in the left ventricle is expelled with each heartbeat. The ejection fraction of a normal heart is between 55 and 70 percent but can decrease by up to 10% in severe heart failure.
It is important to note, however, that about half of patients are categorized as having heart failure with preserved ejection fraction (HfpEF), meaning that the heart muscle has become so thick and stiff that it is no longer able to expand adequately when the ventricle fills and therefore contains a smaller volume of blood than usual. The heart may then have an approximately normal ejection fraction, around 50% for example, but the total quantity of blood pumped with each beat is nevertheless reduced and is not sufficient to meet the body’s needs. The majority of HfpEF heart failure patients are also overweight or obese and several studies (here, for example) suggest that this excess weight contributes to the development and progression of this type of heart failure.
In this study, researchers recruited 529 obese patients (mean BMI 37) with heart failure with preserved ejection fraction (HfpEF) and treated them for one year with a placebo or semaglutide (2.4 mg per week). The results are quite impressive, both in terms of body weight lost by patients treated with semaglutide (nearly 15%) and the improvement in certain parameters associated with heart failure, such as a reduction in the symptoms of the disease and improvement in the functional status of patients (Figure 4).
As noted by the experts, the 8-point difference in the KCCQ-CSS score observed between semaglutide and placebo is very significant, 2 to 4 times greater than what is typically observed in trials with other drugs. More than 50% of patients treated with semaglutide even increased their score by 15 points, which corresponds to a clear improvement in their clinical condition. These beneficial effects of semaglutide were directly correlated with patients’ weight loss, regardless of their degree of obesity (BMI of 30 to 40 or more) or their ejection fraction (45 to 60% or more) at baseline.
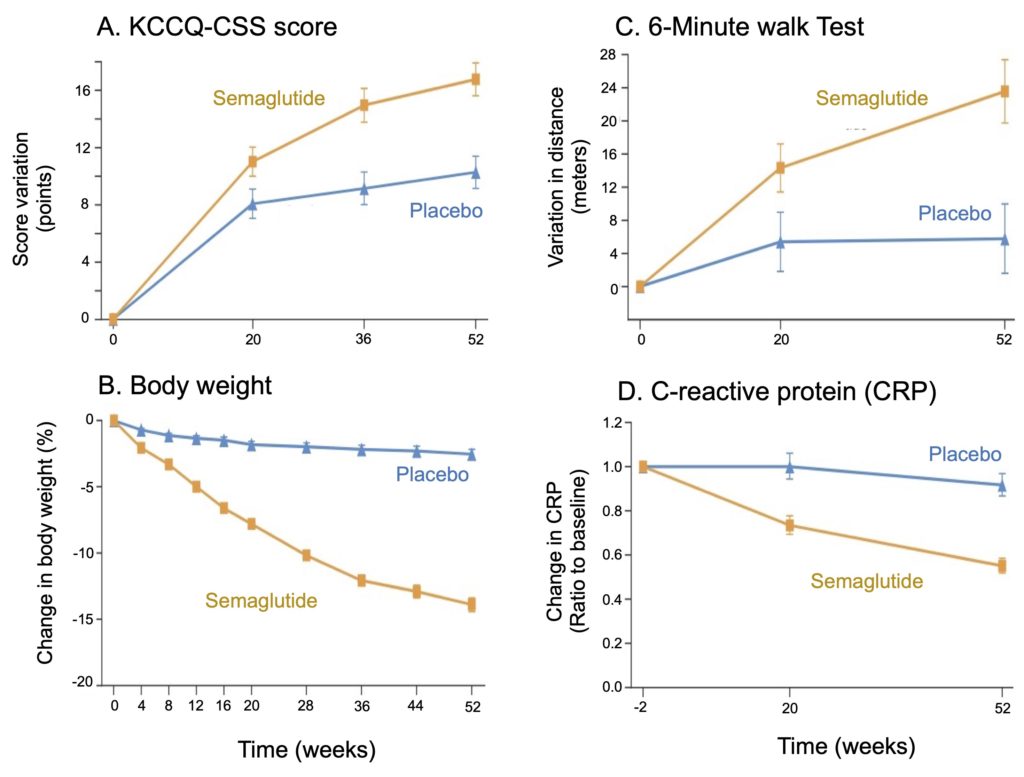
Figure 4. Changes observed in heart failure patients treated with placebo or semaglutide. A. The Kansas City Cardiomyopathy Questionnaire-clinical status summary (KCCQ-CSS) is used to estimate the severity of heart failure in terms of disease symptoms (fatigue, dyspnea, edema) and its physical limitations on daily life (physical, emotional, social). An increase in points in this score corresponds to an improvement in the clinical status of patients, which is more pronounced in those who received semaglutide. B. The weight losses observed during the study are expressed as a % of the initial body weight of the participants, which was around 105 kg on average (BMI = 37). Note the very significant weight loss associated with treatment with semaglutide. C. The walk test measures the distance covered by participants over a 6-minute period, averaging around 300 metres. A greater distance here again reflects an improvement in the functional status of patients treated with semaglutide. D. C-reactive protein is an inflammatory protein, and its decrease reflects a reduction in chronic inflammation in patients treated with semaglutide, which could contribute to the improvement in the clinical status of patients. Adapted from Kosiborod et al. (2023).
Obesity is therefore not simply a comorbidity of heart failure, but a metabolic cause that contributes to the development of this disease. The possibility of substantially improving the clinical status of heart failure patients using these new generation anti-obesity drugs therefore represents a huge step forward in the management of this extremely debilitating and difficult-to-treat condition.
SELECT study
The second study (called SELECT) on the cardiovascular effects of semaglutide treatment focused on the prevention of cardiovascular events in obese patients with a history of cardiovascular disease and therefore at a very high risk of recurrence (Figure 5). After an average follow-up of 40 months, there was a statistically significant 20% reduction in the primary endpoint (a combination of heart attack, stroke, and cardiac death) in patients treated with semaglutide compared to those treated with placebo (Figure 5A). In absolute numbers, however, this protective effect is much less impressive, with a reduction of only 1.5% in the incidence of cardiovascular events. In other words, only 1-2 obese patients at very high risk of recurrence out of 100 can benefit from the positive effect of the molecule, even after 3 full years of treatment. This result falls far short of expectations, especially considering the high cost of this new class of drug.
It should be noted, however, that the weight losses achieved during the SELECT study are much lower than those reported in the study on heart failure mentioned earlier (see Figure 4) and in several other clinical trials (see our article on the subject). Instead of average weight losses of around 15%, SELECT patients lost approximately 8.5% (subtracting placebo) of their body weight (Figure 5B), and it is questionable whether greater weight loss could have further reduced the risk of cardiovascular events in these patients. The arrival on the market of new anti-obesity drugs generating greater weight loss, notably tirzepatide (recently approved under the name Zepbound), could help answer this question.
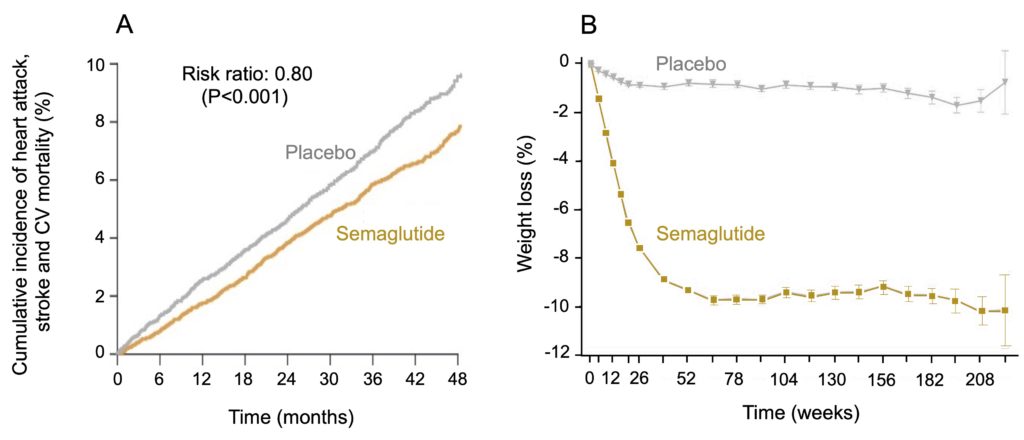
Figure 5. Effect of treatment with semaglutide on the risk of cardiovascular events in the SELECT study. The 17,605 participants in the study (mean age 62 years, mean BMI 33 kg/m2) were treated with semaglutide or a placebo and followed for an average duration of 40 months. The patients were not diabetic, but nevertheless presented abnormal levels of HbA1c (5.7-6.4%), a marker of chronic hyperglycemia, had a history of cardiovascular disease (infarction, stroke, peripheral arterial disease), and were therefore at high risk of recurrence despite aggressive medication (statins, anti-platelets, antihypertensives). A. Treatment with semaglutide is associated with a 20% reduction in the risk of cardiovascular events (a combination of heart attack, stroke and cardiovascular mortality), which corresponds, however, in absolute numbers, to a reduction of only 1.5% in the incidence of these events. B. Weight loss, expressed as a % of initial body weight, following treatment with semaglutide averages approximately 9% and peaks at 1 year. From Lincoff et al. (2023).
Overall, the results of these studies confirm that for people who suffer from obesity, body weight loss is associated with an improvement in their cardiovascular health. This is particularly evident in those with heart failure, and there is no doubt that these people can greatly benefit from these new generation anti-obesity drugs. However, the SELECT study revealed that these benefits are much more uncertain in secondary prevention in patients at very high risk of recurrence, and there is still no data available in primary prevention in obese people with no history of cardiovascular disease. With the exception of heart failure, it is therefore still much too early to determine whether these drugs could eventually represent a valid therapeutic option to improve the cardiovascular health of the overweight population. Especially since these molecules are not without side effects that are sometimes quite significant, particularly at the gastrointestinal level: in addition to nausea, which is very common, a recent study reported that GLP-1 agonists increase by 10 times the risk of pancreatitis and by 4 times the risk of intestinal obstruction and gastroparesis (slowing down or stopping the transport of food from the stomach to the intestines).
Prevention rather than cure
A huge limitation of the treatment of obesity using these new generation drugs is that currently available data indicate that stopping treatment quickly leads to a regain of the majority of the weight initially lost. In other words, treatment with these drugs could be “lifelong”, much as is currently the case for hypertension or high cholesterol. This raises many concerns, both in terms of their long-term effects on health and from a financial point of view. In Quebec, for example, it is estimated that around 28% of the adult population is obese, which corresponds to nearly 2 million people. Since a year of treatment with these drugs costs around $6,000 per person, this means an annual bill of around $12 billion.
As with all lifestyle-related diseases, the solution to the obesity epidemic lies much more in prevention than in treatment. Data accumulated in clinical trials with new anti-obesity drugs clearly show that it is the loss of appetite, particularly for high-calorie foods, that plays a central role in weight loss. In other words, the significant increase in the number of overweight people observed in recent decades is caused by overconsumption of food and not by an excessively sedentary lifestyle, as we often hear.
In terms of prevention, this means that it is essential to improve the dietary habits of the population if we hope to reduce the incidence of obesity and the many chronic diseases that result from it. The means exist and could be implemented with a little political will: nutritional labelling on the front of packaging to clearly identify products containing too much sugar, fat or salt; taxing sugary drinks to encourage consumers to choose healthier options; expanding access to locally grown fruits and vegetables while supporting local businesses. This is particularly important to eliminate excess weight in children and adolescents, which has risen sharply in recent years, as it is well established that childhood obesity dramatically increases the risk of becoming obese as an adult.