Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesSmoking remains a leading cause of premature death worldwide due to the many serious diseases that disproportionately affect smokers, particularly cardiovascular (heart attack, stroke) and pulmonary (lung cancer, chronic obstructive pulmonary disease) diseases (Figure 1).
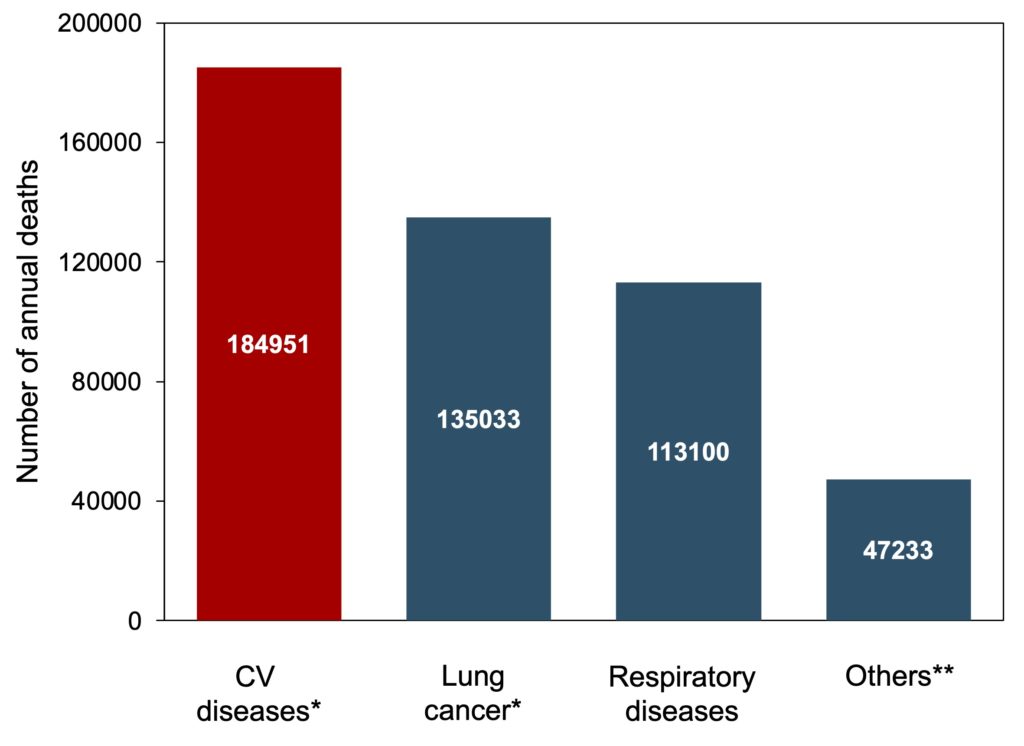
Figure 1. Annual smoking-related mortality in the United States, 2005–2009. Of the 480,317 annual tobacco-related deaths, nearly 40% are due to cardiovascular disease, particularly coronary heart disease (133,251 deaths). *Values include deaths related to second-hand smoking. **Deaths caused by other tobacco-related diseases, particularly various cancers (bladder, mouth, larynx, esophageal, etc.). Source: Centers for Disease Control and Prevention.
The close link between smoking and the development of cardiovascular disease is particularly well-established, with several studies showing that the risk of myocardial infarction is overall 2-3 times higher in smokers than in non-smokers, and even much higher in heavy smokers (one pack or more per day) (Figure 2). It has also been observed that the risk of sudden cardiac death is 10 times higher in smokers. There is therefore clearly nothing worse than tobacco for cardiovascular health and, for smokers, quitting smoking remains the most effective intervention to reduce the risk of serious cardiac events.
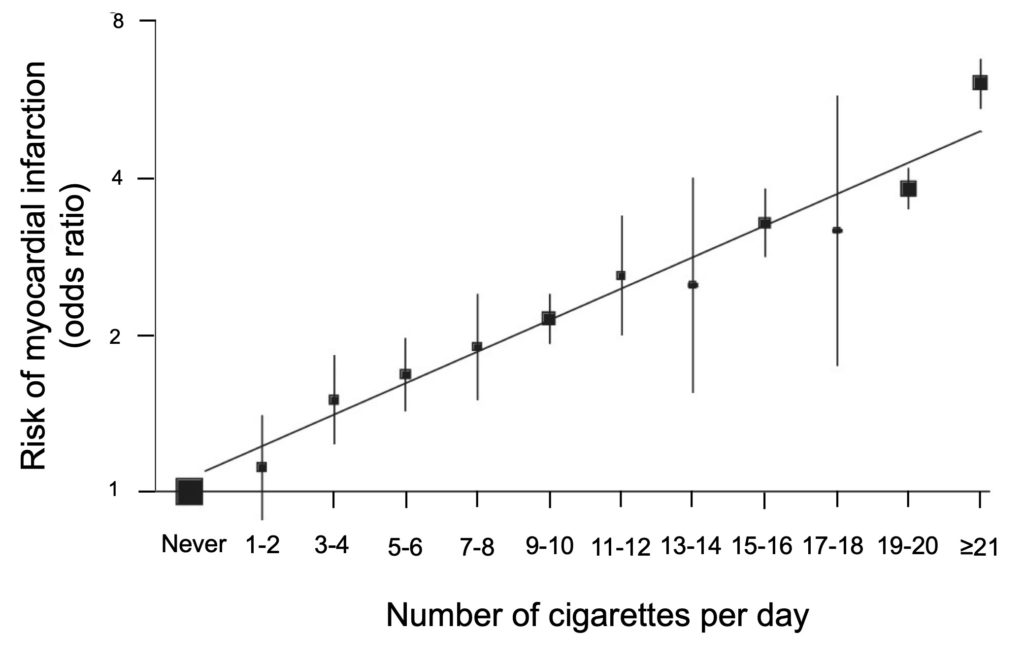
Figure 2. Increased risk of heart attack according to the number of cigarettes smoked per day. For each additional cigarette, the risk of myocardial infarction increases rapidly (risk doubled from 7-8 cigarettes per day) and continues to increase significantly thereafter to reach 6 times for smokers of a pack per day and even 9 times for very heavy smokers (≥ 40 cigarettes per day). Adapted from Koon et al. (2006).
Post-infarction smoking
The importance of quitting smoking is even more urgent for smokers who have had a heart attack and have undergone revascularization to restore blood flow to the heart, either by angioplasty (placement of stents that widen the arteries) or by coronary artery bypass grafting. Studies show that smokers who continue to smoke after undergoing either procedure are at higher risk of restenosis (recurrence of the artery blockage) and of having another heart attack. Smoking also reduces the effectiveness of antiplatelet agents given to patients who have undergone revascularization, which contributes to the increased risk of complications in persistent smokers.
The negative effect of smoking is particularly well-documented by studies on the risk of mortality after angioplasty, the most frequently used procedure to treat heart attacks or severe angina (approximately 50,000 procedures annually in Canada). For example, a ten-year follow-up of smoking patients who underwent angioplasty showed that those who continued to smoke after the procedure (almost 2/3 of the patients in this study) had a significantly lower probability of survival than those who had quit smoking immediately after treatment (Figure 3). When these survival rates are compared to those of non-smoking patients, there is a 76% increase in the risk of premature mortality in persistent smokers, while this increase in risk decreases to 21% in those who quit smoking after angioplasty. Quitting smoking after a heart attack is therefore essential to improve patients’ chances of long-term survival.
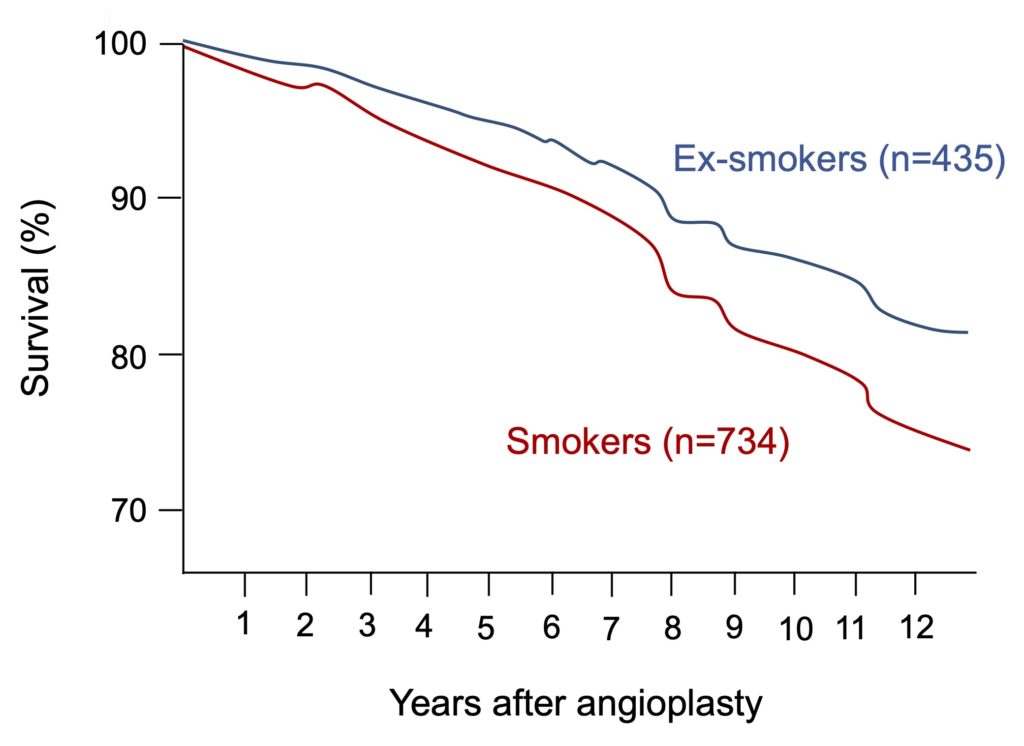
Figure 3. Comparison of the survival curves of smokers who have quit smoking or not after angioplasty. Persistent smokers (red line) are patients who smoked before and after angioplasty, while ex-smokers (blue line) are those who quit smoking immediately after the procedure. Adapted from Hasdai et al. (1997).
Vaping to quit smoking
In recent years, e-cigarettes have established themselves as one of the best tools available to quit smoking, with a quit rate about twice as high as that of approaches using traditional nicotine substitutes (patches, gum).
Another advantage of the electronic cigarette is that it drastically reduces exposure to tobacco toxic compounds and therefore represents a very interesting alternative for highly dependent smokers who have great difficulty quitting smoking. Let us remember that this strong dependence on tobacco is due to nicotine, but that it is rather the 7,000 chemicals compounds produced during the combustion of tobacco that are responsible for the health problems linked to smoking (nicotine does not have any major negative effects on health). By allowing the inhalation of nicotine without the toxic compounds present in cigarette smoke, the electronic cigarette makes it possible to reproduce to a large extent the benefits associated with quitting smoking.
This seems to be particularly true with regard to cardiovascular health. For example, a randomized clinical study observed that the transition from tobacco cigarettes to e-cigarettes was associated with a rapid improvement in vascular health (endothelial function, arterial stiffness). Another study showed that vapers had a much lower risk of cardiovascular events than tobacco cigarette smokers and even similar to that of non-smokers. Given the catastrophic effect of tobacco on the health of patients who have undergone angioplasty, it is therefore possible that the transition of these smokers to e-cigarettes after the procedure could reduce the risks of complications and improve their survival.
Post-angioplasty vaping
This possibility was recently examined in a Korean study of 17,973 adults who smoked an average of 20 cigarettes per day at the time of angioplasty to treat a heart attack or angina. After surgery, patients were followed for about 5 years to measure the incidence of major cardiovascular events (a combination of sudden death, myocardial infarction, and additional angioplasty) in those who continued to smoke, those who successfully quit, and those who replaced tobacco cigarettes with e-cigarettes.
Unsurprisingly, the results show that persistent smokers are the patients most at risk of developing post-angioplasty complications, with nearly 1 in 5 people affected by a cardiovascular event in the first years following the procedure. On the other hand, the study clearly shows that the incidence of these complications is significantly reduced both in patients who stopped smoking and in those who replaced tobacco cigarettes with e-cigarettes (Figure 4).
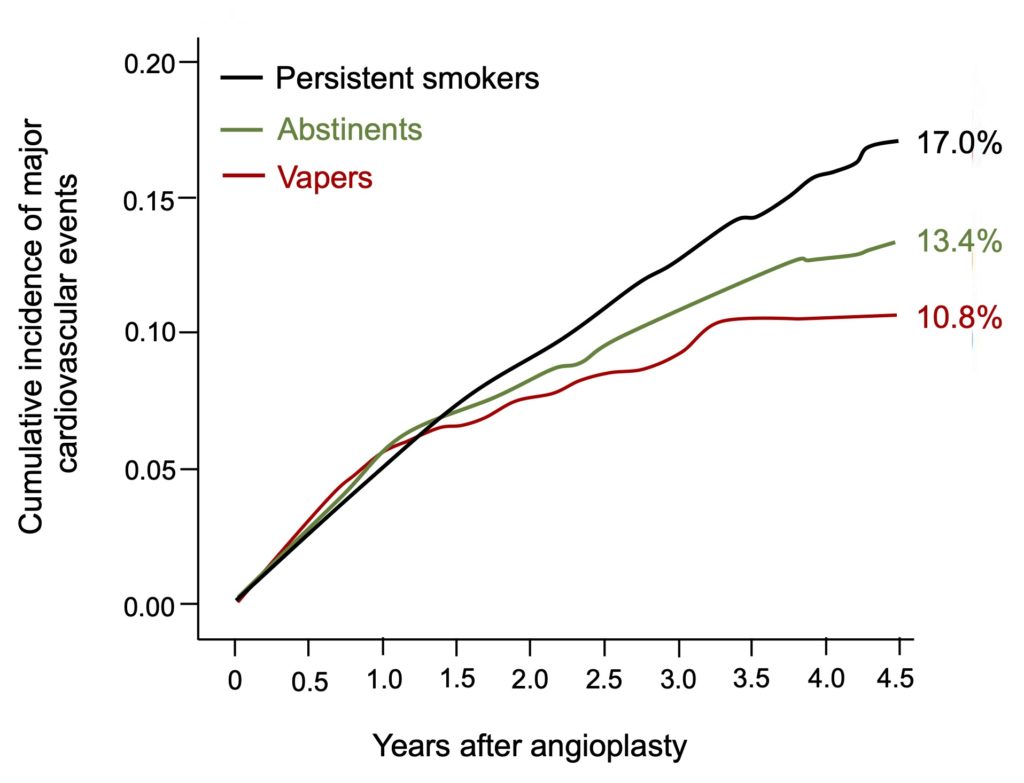
Figure 4. Comparison of the incidence of major cardiovascular events according to changes made by smokers following angioplasty. Of the 17,973 patients who smoked before angioplasty, half of them (8,951 people) continued to smoke after the procedure, 41% (7,328 people) managed to quit smoking completely and 9.5% (1,694 people) used e-cigarettes as an alternative to tobacco. Note the significant decrease in post-angioplasty cardiovascular events (a combination of mortality, myocardial infarction, and additional angioplasty) in both abstainers and vapers compared with persistent smokers. Adapted from Kang et al. (2024).
This positive effect of e-cigarettes is even more pronounced when the analysis is restricted to exclusive vapers, i.e. those who have completely eliminated cigarettes and use e-cigarettes as their sole source of nicotine (Figure 5). This is in line with previous studies that have shown that dual users (tobacco and e-cigarettes) are exposed to a higher amount of toxic substances and remain at greater risk of cardiovascular events than exclusive vapers. It therefore appears that to be truly effective in terms of harm reduction, e-cigarettes must be a substitute for tobacco and not simply a complement, for example to obtain a dose of nicotine when smoking cigarettes is not possible.
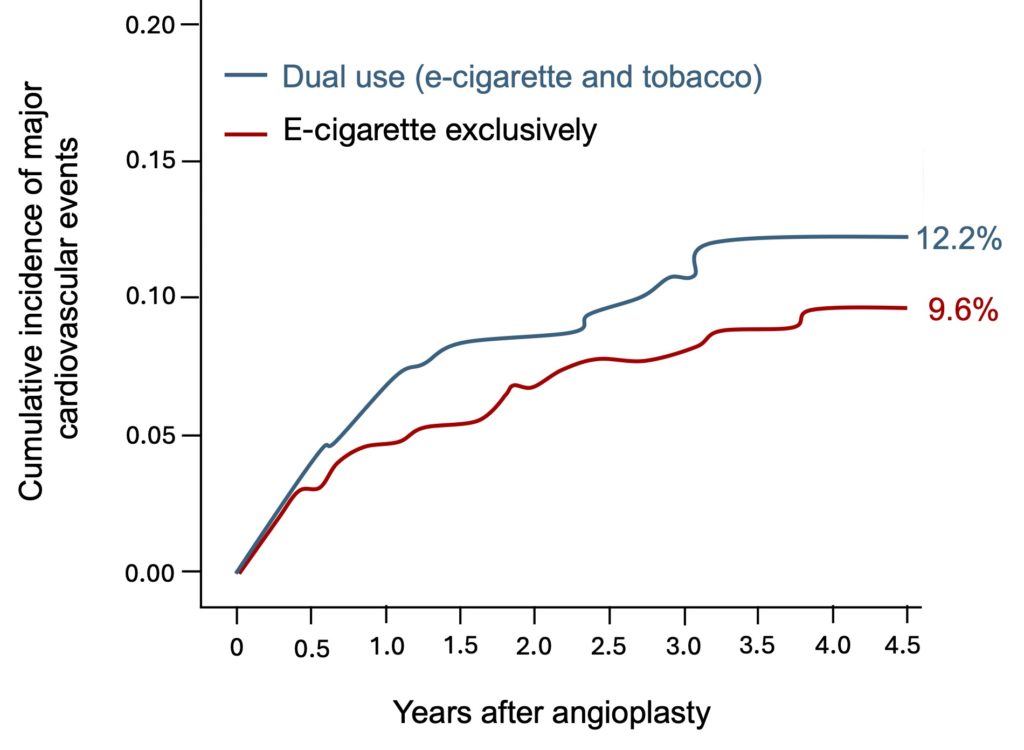
Figure 5. Comparison of the incidence of major cardiovascular events between exclusive vapers and dual users. After angioplasty, approximately half of vapers permanently switched from tobacco cigarettes to e-cigarettes, while the other half used both modes of nicotine delivery. Note the greater decrease in the incidence of cardiovascular events among exclusive vapers. Adapted from Kang et al. (2024).
Although quitting smoking after a cardiovascular event should be considered a medical emergency, a large proportion of patients continue to smoke because of their high nicotine dependence. The demonstration that using e-cigarettes is as effective as quitting smoking altogether in reducing the risk of post-angioplasty complications is excellent news in this sense, because regular nicotine intake can greatly facilitate quitting smoking in highly dependent smokers and thus substantially improve their chances of survival.