Dr Éric Thorin, Ph. D.
Professeur titulaire, Département de Chirurgie, Université de Montréal. Chercheur au centre de recherche de l'Institut de cardiologie de Montréal.
See all articlesOverview
- In Canada, myocardial infarction is the leading cause of death in both men and women.
- However, there are notable differences between the two sexes: men develop atherosclerosis, the disease that causes heart attacks, ten years earlier than women and are at greater risk of premature death.
- On the other hand, when a heart attack occurs before the age of 65, the risk of death for women is almost twice that of men.
- In recent decades in Quebec, the annual incidence of heart attacks has been increasing in women, but decreasing in men.
- Recent data suggest that atherosclerosis is very different in women, but the impact of these differences on the management of the disease are still unknown.
We have long known that men and women (biological sex male and female) are not equal in the face of disease and that there are enormous differences in the incidence of several diseases according to sex (Table 1).
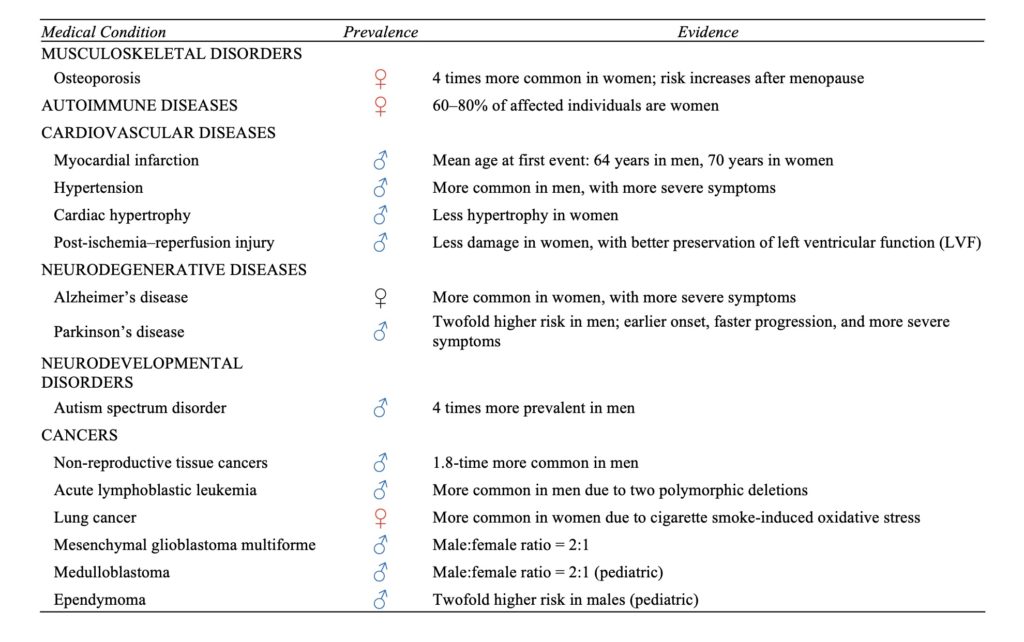
These differences begin very early in life, during embryonic development, when sex chromosomes strongly influence the molecular structure of cells; not in their physiological function as such—a muscle cell, for example, will contract, and this occurs in both sexes—but rather in their capacity to repair cellular damage caused by their metabolic activity. These differences appear from the outset, well before sex hormones—estrogen, progesterone, testosterone—come into play, but evidently these hormones will reinforce the differences between the two sexes at puberty.
Cardiovascular diseases are one of the best examples of this difference in susceptibility between the sexes. Although myocardial infarction is the leading cause of death in both men and women, a significantly higher number of men (nearly 16%) than women (approximately 12%) die from a heart attack each year (Table 2). Therefore, it appears that even though the wear and tear on large blood vessels caused by the sudden increase in blood pressure with each heartbeat is inevitable, this wear and tear seems to be accelerated in men compared to women. This is clearly demonstrated by a recent study which observed that men developed cardiovascular disease on average seven years earlier than women.
| Rang | Femmes | % | Hommes | % |
|---|---|---|---|---|
| 1 | Myocardial infarction | 12.3 | Myocardial infarction | 15.7 |
| 2 | Alzheimer’s disease | 8.6 | Lung cancer | 7.6 |
| 3 | Lung cancer | 7.3 | Stroke | 4.9 |
| 4 | Stroke | 7.0 | Chronic obstructive pulmonary disease | 4.8 |
| 5 | Chronic obstructive pulmonary disease | 5.2 | Alzheimer’s disease | 4.1 |
| 6 | Breast cancer | 4.4 | Prostate cancer | 3.8 |
| 7 | Colorectal cancer | 3.7 | Colorectal cancer | 3.7 |
| 8 | Falls | 3.6 | Chronic kidney failure | 2.8 |
| 9 | Chronic kidney failure | 3.3 | Falls | 2.7 |
| 10 | Respiratory infections | 2.7 | Drugs | 2.7 |
Table 2. Top ten causes of death and the percentage of total deaths they represent in Canada by biological sex. For year 2023; Institute for Health Measurement and Evaluation.
History and chronology of atherosclerotic coronary artery disease in men and women.
In 1772, the English physician William Heberden described angina pectoris, a sign of coronary artery obstruction that could lead to a heart attack, and noted, “I have seen about a hundred people with this disorder, of whom there were only three women.” In 1896, Sir William Osler, a renowned Canadian physician, gave a lecture at Johns Hopkins University, and quoting Heberden, added, “In my own series of 40 cases of true angina, there was only one woman.” Clearly, these two esteemed physicians treated only wealthy clients, who were thus protected from unsanitary conditions and malnutrition. Life expectancy at birth in Dr. Osler’s time, although somewhat improved since Dr. Heberden’s era, was still around 40 years, as the majority of the population died young from infections resulting from nutritional deficiencies and an unhealthy environment. Angina, therefore, afflicted upper-class men in their fifties who lived in a healthy environment, ate well (too well), exercised little, and smoked cigars while their wives retired to the drawing room for a cup of tea!
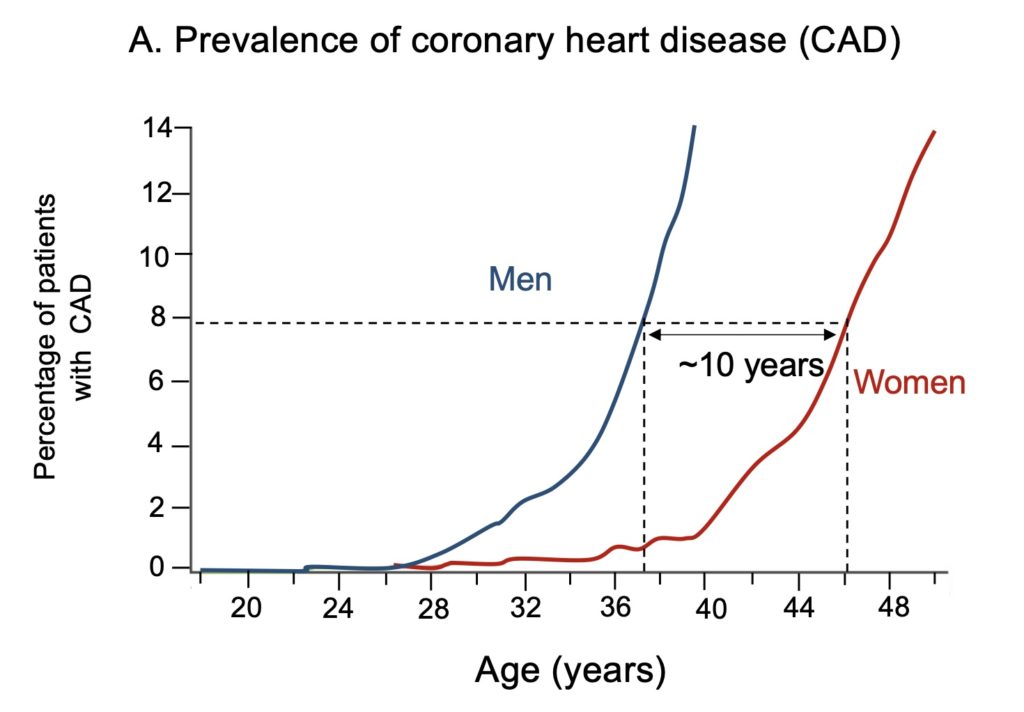
We now know that this difference in susceptibility to cardiovascular disease between men and women is only temporary; a decade before menopause and the loss of protection seemingly provided by optimal ovarian function and estrogen production—its concentration begins to fluctuate significantly in the fourth decade—the risk of myocardial infarction skyrockets in women and becomes almost as frequent as in men. The main difference between men and women, therefore, lies in the rate of development of atherosclerosis, the process of accumulation of lipid-rich plaques in the artery walls. The first signs of this atherosclerosis, atheromatous plaques, are visible as early as their twenties in both men and women (Fig. 1A). But in the latter, the number of cases is very low and remains fairly stable until the age of 40, after which its prevalence (total number of cases in the population) increases almost as rapidly as in men.
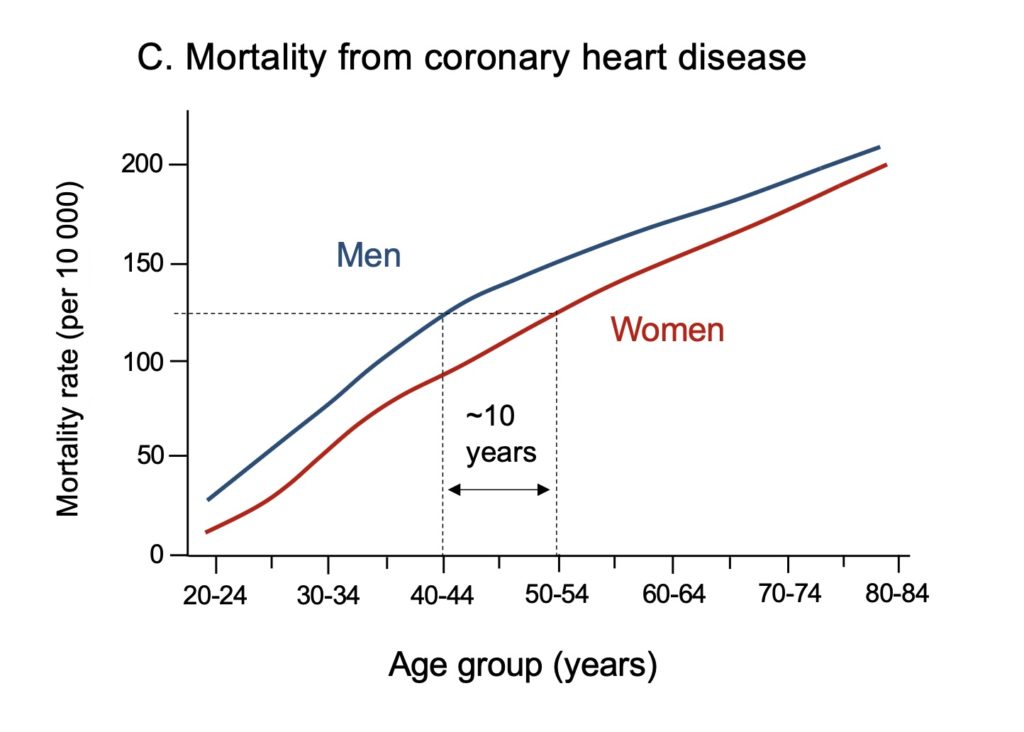
This cardiovascular protection provided by the ovaries and estrogens is therefore crucial in women. In men, the acceleration of atherosclerotic disease cases thus began ten years earlier, in their thirties (Fig. 1A). This very early appearance of atherosclerotic plaques, a sign of premature wear and tear on blood vessels, is reflected by a decrease in the ability of these vessels to dilate in response to blood flow, a phenomenon that also appears about ten years earlier in men than in women (Fig. 1B). This dysfunction, known as endothelial dysfunction, is recognized as the most predictive sign of a future cardiovascular event. Estrogen is a positive stimulator of endothelial function. The logical impact of premature onset in men of endothelial dysfunction and growth of atherosclerotic plaque inside the coronary arteries is that mortality from infarction, the blockage of these arteries, also occurs ten years earlier in men than in women in North America (Fig. 1C) and in all high-income countries.
What explains this ten-year difference in women’s cardiovascular protection?
The common denominator of cardiovascular protection in women is thus ovarian function and estrogens. In Osler’s time and up until the 1960s, cardiovascular disease risk factors such as hypertension, hypercholesterolemia, and diabetes, to name a few, were not addressed. Since atherosclerosis is a disease that takes decades to develop before becoming symptomatic, the ten additional years of protection available to women were fully realized in their favour, as men could have a heart attack leading to death in their fifties—prematurely, according to our current standards.
Although they have a significant advantage, women are nonetheless exposed to unique risks that influence the onset of cardiovascular disease in adulthood. We now know that diabetes (and smoking) accelerates the risk of coronary atherosclerosis, the disease that causes heart attacks, more in women than in men. Furthermore, women are exposed to pregnancy-related conditions such as gestational diabetes, preeclampsia, and gestational hypertension, which are additional risk factors for the growth of atherosclerotic plaques. Polycystic ovary syndrome, premature menopause, and multiple pregnancies also increase the risk of insulin resistance, dyslipidemia, and obesity—all risk factors for cardiovascular disease. When a woman has a heart attack, she is 75% more likely than a man to die within 30 days, especially at a young age. Why? Good question. We don’t know, or we only have hypotheses.
Lack of knowledge of the basis of atheromatous disease in women.
Historically, the studies that led to the development of drugs to treat cardiovascular diseases were carried out in men, on the one hand because more men than women were afflicted by these diseases (and still are), and on the other hand, because the recruitment of women in clinical studies was greatly slowed down by stricter regulations introduced following the tragedy linked to the use of thalidomide as an anti-nausea in pregnant women in the 1950, which led to very severe congenital malformations in thousands of children. The male sex still remains the medical reference today and very few clinical studies have published their results based on the sex of the subjects. To address this bias, major research funding agencies like the Canadian Research Institutes, the American Heart Association and the European Commission called a little over a decade ago for more awareness and education on sex and gender differences in medicine and health care, and to include more women in large studies. For all these reasons, our understanding of the molecular contribution of biological sex in heart disease is slowly improving but still remains very limited. However, this understanding is essential to the development of better medications.
For example, women respond differently to medications and may experience more side effects, generally due to overexposure of doses and different pharmacokinetics, i.e., the speed at which the medication reaches its peak concentration in the blood and is then eliminated. While overall both sexes respond similarly to current medications used to treat cardiovascular disease, there are some exceptions in specific medical conditions with greater effectiveness in men compared to women.
Recent advances reveal molecular differences in the presentation of atherosclerosis between men and women.
Large-scale studies of the impact of female sex on cardiovascular disease are only just beginning. The initial findings are surprising. The endothelium from which atherosclerotic plaque develops and grows is molecularly and structurally different in men and women. A recent study from the Montreal Heart Institute clearly demonstrates that the molecular signature of the endothelium in the arteries of women with coronary atherosclerosis and a recent myocardial infarction is completely different from that of men with the same medical condition. This difference in men was expected, as scientists have been studying heart disease in males for decades. But the signature in women is surprising: compared to men, women’s endothelium contains fewer senescent cells, less activation of inflammatory and oxidative stress pathways, and a greater capacity to dilate arteries by releasing nitric oxide (NO), despite their advanced age (approximately 68 years in this study). The first unanswered question, therefore, is why do women develop atherosclerotic lesions with such a seemingly protective profile? We do not fully understand all the mechanisms that lead to the disease in women. This is especially true since all the results confirm the greater resilience of women’s endolethial cells, although these women have been menopausal for an average of 15 years and have therefore lost the sustained cardioprotective effect of estrogen for probably nearly 25 years.
Once present, the plaque is also different: studies have revealed structural differences in atherosclerotic plaques, which are more lipidic and less stable in men and more fibrous and structured in women, with highly distinct proteomic (protein) and transcriptomic (mRNA) signatures of the plaque between the sexes. This characteristic of the fibrous structure could contribute to producing a more flexible plaque that is less prone to rupture, which would explain the lower incidence of atherothrombotic events (blood clot formation) in women compared to men. In fact, a recent study shows that there are significant differences in the causes of myocardial infarction between the sexes in patients under 65 years of age; the incidence of myocardial infarction in the general population is lower in women, as previously established, but this difference is particularly pronounced when the infarction is of atherothrombotic origin (23 in women vs. 105 in men per 100,000 people/year). Conversely, the incidence of spontaneous coronary artery dissection (a tear in the artery wall) is much higher in women (3.2 vs. 0.9 per 100,000 people/year) than in men. In this same study, it is surprising to note that the women with atherothrombosis were the same age as the men (55 ± 8 years vs. 54 ± 8 years) and had equally extensive coronary artery disease, but with a greater burden of risk factors (diabetes, hypertension, dyslipidemia, etc.) than the men, which demonstrates once again the greater resistance to damage in women’s cardiovascular systems. To our knowledge, and particularly to the author of this text, we cannot yet explain these differences based on our current scientific understanding.
Why is it urgent to understand?
The example of the disease’s evolution in Quebec provides us with a good basis for reflection. In March 2026, the Quebec National Institute of Public Health (INSPQ) updated its data on the evolution of acute myocardial infarction from 2006 to 2022. This reflects what is happening in all high-income countries. First, it reminds us that in 2022, 60 people were hospitalized daily for a heart attack (21,900 per year) in a population of approximately 9 million people. Among those hospitalized for a heart attack, 54 died each day in the hospital from all causes, meaning not solely from the effects of their heart attack. This represents a death rate four times higher than that of people who have never been hospitalized for a heart attack. Heart attacks are therefore a significant accelerator of mortality, reflecting the essential role played by the cardiovascular system, its heart and blood vessels, in sustaining life and preventing other diseases.
The data is particularly informative regarding the evolution of the disease according to sex. While the proportion of new cases in the general population remained stable compared to 2006, there was a 23% increase in new cases among women aged 50 to 64, but a 16% decrease among men in the same age group. Improvement in men is expected with advances in our knowledge and better management of the disease. But for nearly 25% of women, it’s as if the protection they had previously enjoyed has vanished. Combined with the fact that the risk of death is 1.7 times higher for women than for men after a heart attack in this age group, the cardiovascular health of women is deteriorating. The reasons? They are numerous: cigarette consumption, while stable between the sexes, shows that in 2015-2016 and 2017-2018, women who smoked 1 to 10 cigarettes a day were proportionally more numerous than men; there is also an increase in obesity, which promotes diabetes, sedentary lifestyles, stress, and other poorly understood factors that we will discuss in future articles from this site.
In conclusion, all this data confirms the lower prevalence of cardiovascular disease in women; however, when a woman has a heart attack, she is almost twice as likely to die from it as a man, which explains why heart attacks are also the leading cause of death in women. We have seen that there are molecular bases to these differences, but our current knowledge is still unable to link them to the differential progression of the disease in women. Understanding these links is essential because we have also seen that the medications used, while generally effective, are sometimes less so in women and produce more side effects. Therefore, there is significant research to be done; the good news is that this research is booming.