Dr Martin Juneau, M.D., FRCP
Cardiologue, directeur de l'Observatoire de la prévention de l'Institut de Cardiologie de Montréal. Professeur titulaire de clinique, Faculté de médecine de l'Université de Montréal. / Cardiologist and Director of Prevention Watch, Montreal Heart Institute. Clinical Professor, Faculty of Medicine, University of Montreal.
See all articlesOverview
- Sudden cardiac death that affects senior athletes during exercise is a very rare phenomenon, with an incidence about 100 times lower than sudden death affecting the general population.
- On the contrary, regular exercise is associated with a strong reduction in the risk of sudden death and premature mortality in general.
- The large volumes of exercise performed by senior athletes are associated with an increased risk of certain cardiac anomalies (calcification of the coronary arteries, myocardial fibrosis), but the contribution of these anomalies to the phenomenon of sudden death remains uncertain.
- In the majority of cases, it is rather the presence of an underlying coronary artery disease that is responsible for sudden death affecting athletes, and they must therefore remain attentive to the appearance of unusual symptoms and ensure that they control well-established risk factors for atherosclerosis, such as cholesterol levels, blood pressure and type 2 diabetes.
As the name suggests, sudden cardiac death is defined as death caused by the sudden and unexpected stopping of the heartbeat, usually an hour or less after the onset of the first symptoms. Sudden death is responsible for approximately 50% of deaths from cardiovascular disease and is often the first (and last) symptom of an underlying cardiovascular disease. In Western countries, the incidence of sudden cardiac death ranges from 50–100 events per 100,000 people per year and is caused in approximately 75% of cases by the presence of coronary artery disease (known or unknown), the remainder being mainly of congenital origin (cardiomyopathies, channelopathies). In Canada, for example, it is estimated that sudden cardiac death affects 97 people per 100,000, which corresponds to about 35,000 deaths annually (about 9,000 per year in Quebec), or about 10% of overall mortality (there were 307,132 deaths in Canada in 2020-21).
Sudden death of athletes: A rare phenomenon
Although sudden cardiac death is very common, we mainly hear about this phenomenon when it affects athletes, for example, during a marathon. This is paradoxical, because while it is understandable that the deaths of people in excellent physical shape and in the prime of life might strike the imagination, the heavy media coverage surrounding these deaths can give the impression that the practice of sports activities represents an important risk factor for sudden death, which is absolutely not the case. In fact, it is well established that sudden deaths associated with sports are very rare phenomena, accounting for only about 5% of all sudden deaths that occur each year in the general population.
Despite this low incidence, it is important to understand the factors responsible for these sudden deaths in athletes. A very large number of studies have looked into this question in recent years to better understand the mechanisms involved, of course, but also to determine whether the risk of these premature deaths could be related, at least in part, to the very large volumes of exercise that are required to achieve athletic performance. In other words, can you exercise too much? Is there a limit beyond which the amount of exercise becomes excessive for the heart and can cause damage that will increase the risk of sudden death?
Senior athletes
Sudden cardiac death in sports is defined as death that occurs during or within one hour of the completion of a sports activity. A French study, which has since become a classic, has shown that the vast majority of these deaths affect people aged 35 and over and occur mainly (90%) in the context of leisure sports activities (Figure 1). These senior athletes (master athletes) represent the sub-population most at risk of sudden sports death, especially since this group of people is constantly increasing, with more and more middle-aged people participating in endurance sports. In the United States, for example, the number of people who have completed a marathon has quadrupled over the past 25 years, increasing from 5 to 20 million runners per year, more than half of whom are over the age of 35.
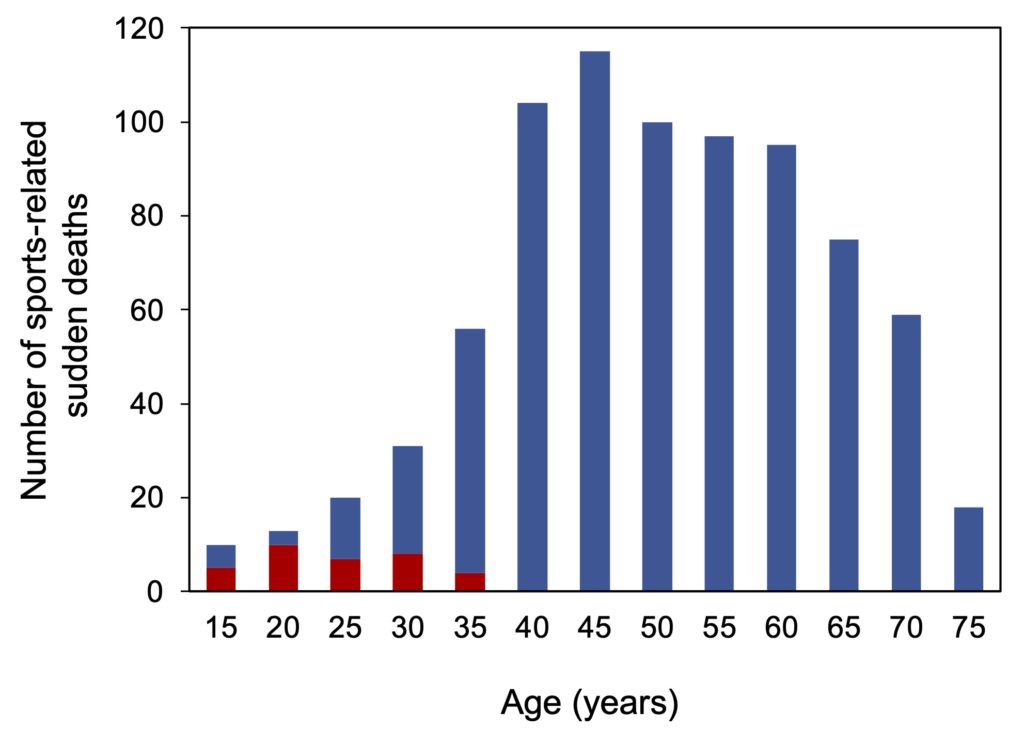
Figure 1. Distribution of sports-related sudden cardiac death by age. The values represent the total number of athletes who died in France during a 5-year period in the general population (blue rectangles) and among young people participating in individual or team organized competitive sports (red rectangles). Note that the vast majority (95%) of deaths occurred among people aged 35 and over. Taken from Marijon et al. (2011).
Men at risk
As mentioned earlier, sudden death caused by intense physical exertion remains a rare phenomenon, with an incidence of about 0.5-1.0 deaths per 100,000 participants, which is about 100 times less than the sudden death that occurs in the general population, outside of a sports context (50–100 per 100,000 people) (Table 1).
Male athletes represent the vast majority of these deaths, with a risk of sudden death 10 to 20 times higher than that observed in women. This difference is observed for all sports activities, including the marathon, and is probably related to the protective effect of estrogen against the development of coronary heart disease, one of the main causes of sudden death (see below).
Table 1. Incidence of sports-related sudden cardiac death, by age and sex.
Note the increased risk of sudden death in older men, especially for triathlon.
*For comparison, the incidence of sudden death observed for the Montreal metropolitan area in 2001 is shown.
| Incidence of sudden cardiac death (per 100,000 participants) |
|||
|---|---|---|---|
| Sport in general | Total | Men | Women |
| All ages | 0.55 | 1.01 | 0.05 |
| 35-54 years | 0.66 | 1.25 | 0.05 |
| 55-75 years | 0.75 | 1.42 | 0.07 |
| Marathon | |||
| All ages (22-65 years) | 0.54 | 0.90 | 0.16 |
| Triathlon | 1.74 | 2.4 | 0.74 |
| 40-49 years | 3.96 | 6.08 | 0.96 |
| 50-59 years | 6.67 | 9.61 | 2.12 |
| ≥ 60 years | 12.9 | 18.61 | 0 |
| Sudden death in general (not related to sport)* | 53 | 66.7 | 39.7 |
The risk of sudden death for male athletes also seems to increase with age (20% increase among those aged 55-75 compared to 35-55-year-olds for sports in general), while women do not seem to be so affected by aging. This impact of age is particularly striking for triathlon, where the risk of sudden death begins to climb as early as age 40 and increases each decade thereafter to become several times higher at age 60 (18.6 per 100,000) than the risk observed for all triathletes (1.74 per 100,000). It should be noted that two thirds of sudden deaths that occur during triathlons occur in the initial swimming stage, which could explain the much higher risk of death during these events than that observed for the marathon. It has been proposed that this higher incidence of sudden death during the swimming event may be due to a combination of several factors, including 1) a sudden rise in catecholamine (adrenaline, noradrenaline) levels caused by the stress of the beginning of the competition; 2) the chaotic start caused by the simultaneous entry of several participants into the water, which causes contact between the competitors and exposure to difficult conditions (big waves, cold water). These factors could play a role in triggering arrhythmias leading to cardiac arrest, especially in people with underlying coronary artery disease.
Overall, sudden sports-related deaths are therefore relatively infrequent and most senior athletes are not at major risk of death during periods devoted to exercise. On the other hand, older men (40 years and over) should be aware that certain very demanding sports, such as triathlon, carry a higher risk of sudden cardiac death.
The exercise paradox
As mentioned earlier, sudden death caused by exertion is most of the time the clinical manifestation of an underlying and asymptomatic coronary artery disease, but which manifests itself suddenly following the significant increase in the workload of the heart during intense exercise. In most cases, the stress imposed on the heart causes the atherosclerotic plaques present inside the coronary arteries to rupture, leading to the formation of thrombi (clots) that block the flow of blood to the heart muscle.
First of all, it should be mentioned that athletes are much less at risk of sudden cardiac death caused by intense exertion than people who are sedentary and therefore less physically fit. Several studies (here, here and here, for example) have indeed reported dramatic increases (17 to 56 times) in the risk of sudden death related to effort in these sedentary people, with in particular an increase in the risk of infarction of up to almost 100 times.
In all cases, however, these large increases in the risk of sudden death are greatly mitigated in people who regularly exercise. This protection is particularly dramatic with regard to the risk of infarction caused by exertion, with a reduction in risk of approximately 50 times observed in people who train regularly, at least 5 times per week (Figure 2). There thus seems to be a certain “exercise paradox”: on the one hand, vigorous exercise can considerably increase the risk of sudden cardiac death in the short term, while, on the other hand, regular exercise confers a strong protection against this risk of sudden death. For example, several studies have shown that just 30 minutes of moderate activity such as walking, 5 times a week, reduces the risk of cardiovascular disease by 20%, a reduction that reaches 30–40% for an equivalent amount of vigorous exercise. The benefits associated with regular physical activity therefore far outweigh the low risk of mortality that can occur during sporting activities.
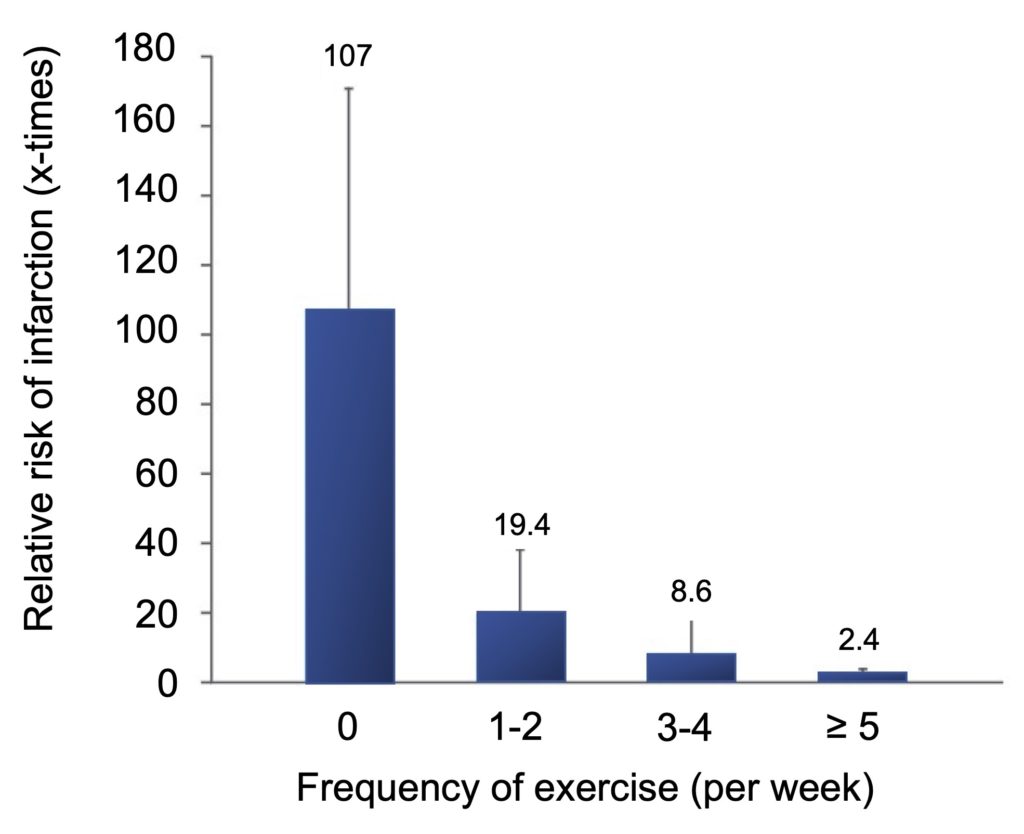
Figure 2. Effect of regular physical exercise on the risk of myocardial infarction caused by vigorous exercise. Taken from Mittelman et al. (1993).
Cap on the health benefits
It is usually recommended to do a minimum of 150 minutes of moderate exercise (e.g., walking) or 75 minutes of vigorous exercise (e.g., running) per week to reap the health benefits of physical activity. It should be mentioned, however, that these recommendations are a little “timid”, as several studies indicate that higher volumes of exercise maximize the reduction in the risk of premature mortality associated with physical activity (Figure 3).
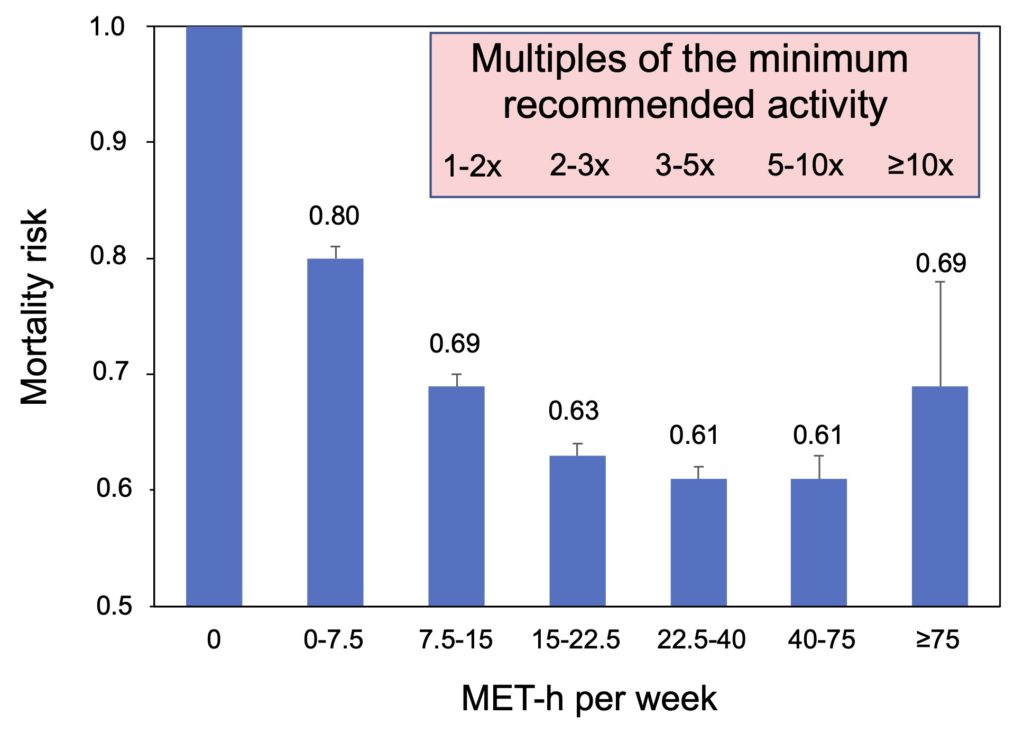
Figure 3. Reduction in the risk of mortality according to the volume of exercise carried out per week. Note the cap of benefits (40% reduction in mortality) observed from a volume of exercise corresponding to 2–3 times the amount recommended by the WHO. Adapted from Arem et al. (2015).
Someone who follows the WHO recommendations to the letter, for example by doing 150 minutes of moderate activity, which corresponds to approximately 7.5 MET-h per week (see the box for the calculation), sees their risk of dying prematurely decrease by 20%. An interesting protection, but which nevertheless remains well below that obtained if the volume of exercise is increased to reach 2 to 3 times the recommended quantities (40% reduction in mortality). On the other hand, it is important to note that there is a limit to the benefits of exercise, since higher volumes of physical activity do not bring additional reductions in mortality, even at amounts 10 times greater than those recommended (Figure 3). As a result, the considerable volumes of exercise that are carried out by senior athletes must above all be considered as sporting feats, often remarkable and beyond the reach of ordinary people, but not as a way to improve health.
Exercise intensity and volume
Exercise intensity is usually expressed as a metabolic equivalent (MET), using resting basal energy expenditure as a benchmark. For example, brisk walking, which is considered moderate-intensity physical activity, causes 3 to 4 times more energy expenditure than sitting still (3 to 4 METs). The energy expenditure of running, which is considered vigorous physical activity, is 6 to 8 times greater than at rest (6 to 8 METs). The volume of exercise performed by a person can be easily calculated by multiplying the duration of the exercise by its intensity. Thus, 150 minutes of moderate activity (4 METs) or 75 minutes of vigorous activity (8 METs) correspond in both cases to a volume of 600 MET-min or 10 MET-h per week.
In the study presented in Figure 3, the greatest reduction in the risk of premature death is observed in people who do 2 to 3 times the recommended amounts of exercise, i.e., 300–450 minutes of moderate activity or 150–225 minutes of vigorous activity (15–22.5 MET-h per week). In concrete terms, these volumes of exercise correspond to approximately one hour of walking or half an hour of running per day.
While the cap on the benefits of regular physical activity on reducing mortality is well established, there is still a gray area with regard to the extremely high volumes of exercise carried out over many years by some senior athletes. In several studies (here, here, here, here, here and here, for example), it is indeed observed that athletes who do enormous amounts of exercise (10 times or more of the recommended amounts) have a risk of mortality slightly higher than those who do it optimally (3 times the recommended amounts) (see for example Figure 3). This diminished benefit is not statistically significant due to the small number of extremely active athletes (typically less than 3% of study participants), but it nevertheless raises the possibility that very large amounts of exercise, repeatedly performed for many years, can exceed the physiological capacities of the body and cause certain damages that reduce the benefits normally associated with an optimal amount of exercise. Sudden deaths affecting athletes despite their great physical condition could therefore be a manifestation of this damage.
Athlete’s heart
It has been observed that very high levels of exercise promote the appearance of three main cardiac abnormalities, namely atrial fibrillation, calcification of the coronary arteries, and myocardial fibrosis. The increased risk of atrial fibrillation in senior athletes is a very well-documented phenomenon, but this electrical disorder does not seem to play a major role in the phenomenon of sudden death in healthy people and so will not be discussed in more detail here.
However, coronary artery calcification and myocardial fibrosis deserve special attention because of the potential contribution of these abnormalities to the two main causes of sudden cardiac death, i.e., cardiac ischemia (blockage of blood supply) and ventricular arrhythmia (dysregulation of electrical signals allowing the orderly contraction of the heart).
Calcification of the coronary arteries. Coronary artery atherosclerosis is the leading cause of sports-related sudden cardiac death, both in the general population and in athletes, including high-level athletes such as marathon runners. A frequently used method to visualize these plaques is to measure the presence of calcium in the coronary wall by cardiac computed tomography (CT scan) and multiply the area by the signal density to obtain what is called a calcium score (CAC score). These scores have some prognostic value: a score between 1 and 100 is associated with a probability of 13% of cardiovascular events over the next 3 years, a risk that reaches 16% for scores 101–400 and 34% for scores >400.
This approach was used to compare the degree of coronary artery calcification of 284 men with an average age of 55 years based on the usual amount of exercise carried out each week since the age of 12 years. The results show that 68% of the most active participants throughout their life (>2000 MET-min per week, which is equivalent to approximately one hour of running each day) had a calcium score greater than zero, compared to only 43% in those who were moderately active (<1000 MET-min per week) (Figure 4).
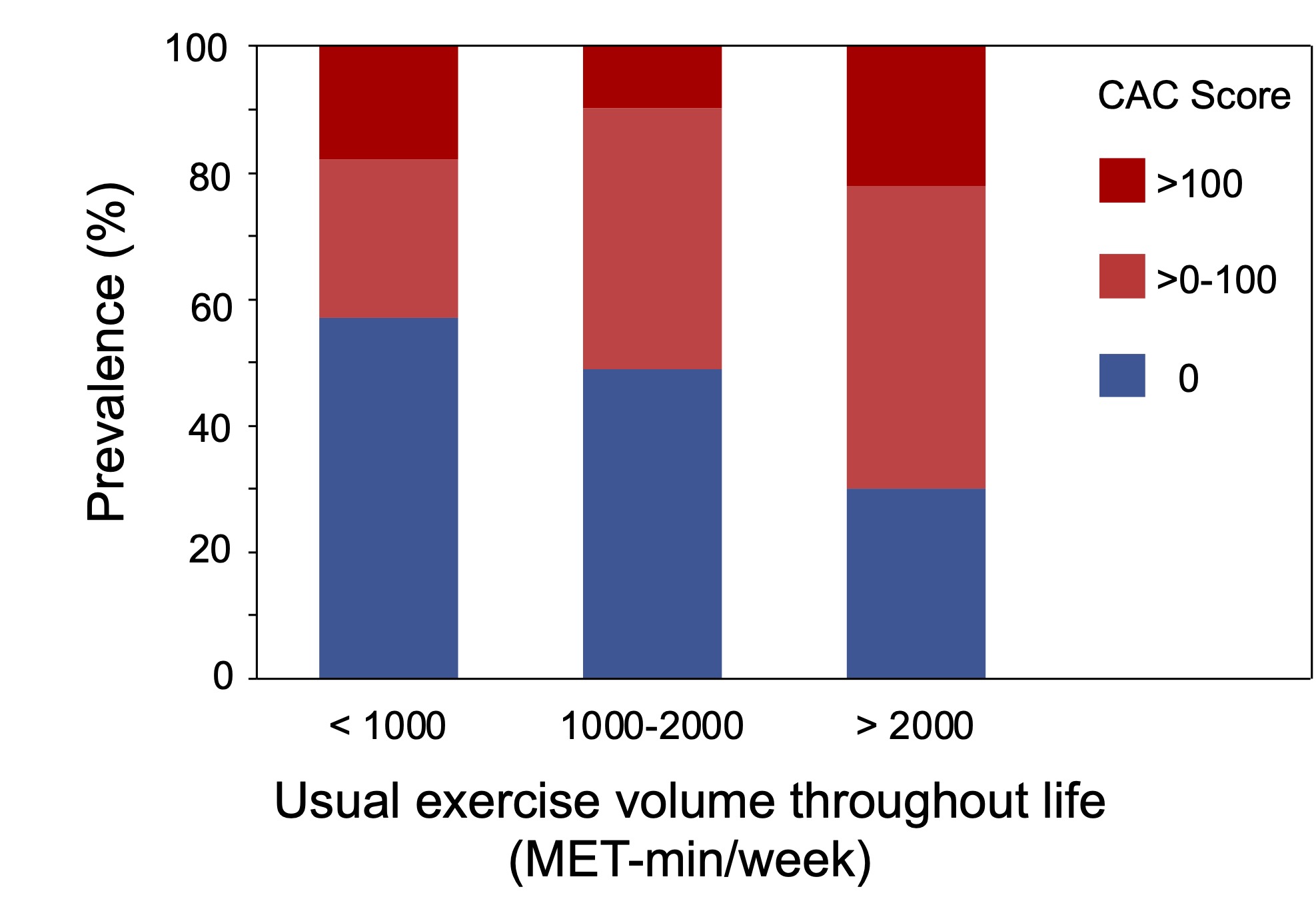
Figure 4. Comparison of the prevalence of coronary artery calcification according to the amount of exercise performed each week over several years. Note the increase in the percentage of athletes with a calcium score greater than zero (red rectangles) for higher volumes of exercise (>2000 MET-min per week for more than 30 years). Taken from Aengevaeren et al. (2017).
In the same vein, a study carried out among senior athletes (over 40 years old) who had practised a very intensive training program for at least 10 years (more than 16 km of running or 50 km of cycling per day, with participation in at least 10 endurance competitions such as marathons and half-marathons) showed that these athletes had a higher prevalence of atherosclerotic plaques in the coronary arteries than men in the control group who exercised much less (44% compared to 22%). In this study, high CAC scores (>300) were observed only in athletes, as well as a significant narrowing (≥50%) of the diameter of the arteries (stenosis) and the presence of this narrowing in more than one vessel. Similar results have also been observed in marathon runners over the age of 50, and so it seems increasingly clear that high amounts of exercise are closely correlated with a higher prevalence of atherosclerotic plaques in the coronary arteries. A very athletic lifestyle therefore does not prevent the development of atherosclerosis, both in the coronary and peripheral arteries.
However, the very low prevalence of sudden cardiac death (and cardiovascular events as a whole) observed in senior athletes suggests that this acceleration of atherosclerosis is not as risky as in the general population. On the one hand, studies indicate that the majority of calcified plaques found in athletes are present in a stable form, unlikely to crack and form a thrombus (clot) blocking the coronaries. In other words, a higher calcium score in an athlete would not have the same prognostic value as a score of the same value in a sedentary individual. On the other hand, the physiological adaptations associated with regular exercise (increased diameter and elasticity of vessels, among others) improve coronary blood flow, which would allow athletes to be less affected by the presence of stenoses and thus avoid coronary events that would affect most people with a similar degree of atherosclerosis.
That being said, atherosclerosis still remains an important cardiovascular risk factor and it would be premature to conclude that the increased presence of plaques in the coronaries of athletes has no impact on their health. In this sense, it should be noted that a follow-up of marathon runners after 6 years showed that an increase in the calcium score is nevertheless associated with an increased risk of cardiovascular accidents in these athletes, going from 1% for scores <100, to 12% for scores of 100–400, and to 21% for scores >400. This is consistent with a study showing that the cardiac arrests suffered by marathon runners during an event were largely caused by an underlying coronary disease that caused an insufficient supply of blood to the heart (ischemia) to sustain the effort. On the other hand, and contrary to what is observed in the general population, none of these ischemia had been caused by a rupture of the atherosclerotic plaques. Overall, it therefore seems that atherosclerotic plaques are indeed more stable in athletes and that their rupture does not represent a major risk of ischemia and sudden death. However, in some athletes, the presence of these plaques can still reduce blood flow to the heart and cause cardiac arrest during sustained and intense effort.
The contribution of coronary artery calcification to the phenomenon of sudden death associated with sports should therefore not be overlooked, even in athletes who display exemplary physical fitness. This is especially true for those who have “converted” to sports later in life, after being exposed for several years to factors that accelerate the development of atherosclerotic plaques, in particular smoking and poor diet. Since atherosclerosis is a generally irreversible process, the burden of plaques that have accumulated during the period preceding the adoption of a more athletic lifestyle remains present and can be expressed in the event of intense and sustained effort. It is thus important to remain attentive to certain signals that could suggest the presence of an underlying coronary disease (unusual shortness of breath, palpitations, pain in the chest, arms or throat). Moreover, it should be noted that about half of senior athletes who suffered a sports cardiac arrest had experienced symptoms in the month preceding the cardiac event.
Myocardial fibrosis. Intense and prolonged exercise (marathon) was observed to be associated with a significant increase in the blood levels of certain markers of damage to cardiac cells (troponin, natriuretic peptide type B) and with dysfunction (reduction in ejection fraction) of the right ventricle (RV) of the heart immediately after the test. This reduction in RV function in response to very intense exercise has been observed in several other studies (see this meta-analysis), suggesting that this area of the heart is particularly at risk of being damaged by very high levels of exercise performed repeatedly and over long periods of time.
These myocardial injuries cause cell breakage and the appearance of fibrotic areas that can be visualized by cardiac magnetic resonance using the late gadolinium enhancement (LGE) technique. A contrast product (gadolinium) is injected and rapidly eliminated from the normal myocardium, but persists longer in the fibrotic areas. By acquiring images more than 10 minutes after the injection, the signal obtained late makes it possible to identify areas of fibrosis.
An analysis of 19 studies involving a total of 509 healthy endurance athletes found that approximately 6% of athletes had a positive LGE signal, indicative of myocardial fibrosis. Studies that have compared LGE in endurance athletes with that affecting less active people (physical activity equal to or lower than the recommendations) show that fibrosis is much more frequent in athletes, with a prevalence of 12% compared to only 1.5%. More recently, a meta-analysis of 12 studies (1350 participants) estimated that the risk of fibrosis is increased by about 7 times in endurance athletes compared to sedentary or less active people (Figure 5).
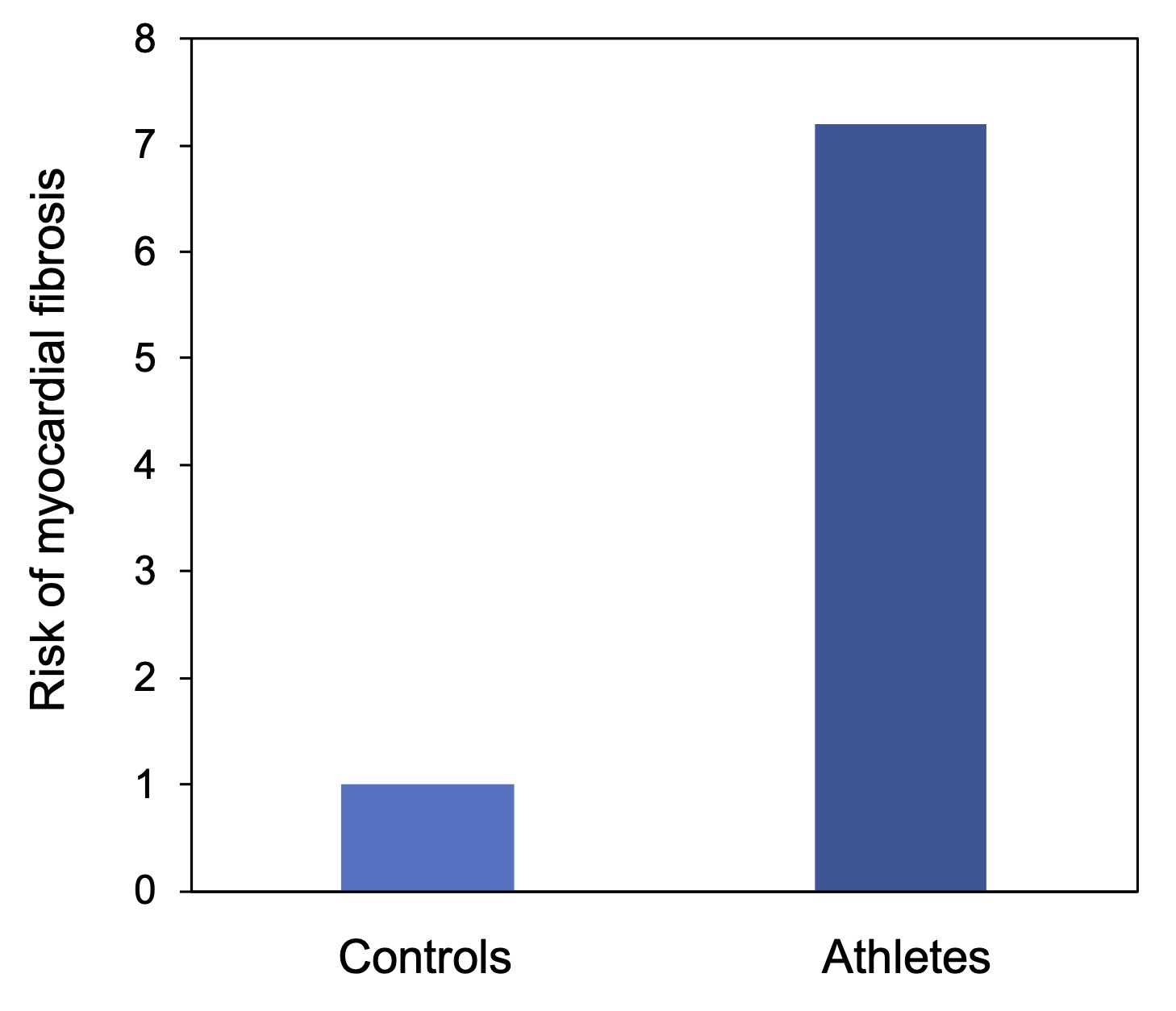
Figure 5. Increased risk of myocardial fibrosis in senior athletes. Athletes who perform large volumes of exercise over several years have a significantly higher LGE signal than controls who exercise 3 hours or less per week. Taken from Zhang et al. (2020).
This higher prevalence of the LGE signal (and therefore of fibrosis) in athletes is strongly correlated with the number of years of intensive training as well as the number of endurance competitions completed, which strongly suggests that large volumes of high-intensity exercise represent a risk factor for myocardial fibrosis. As mentioned before, the right ventricle seems more sensitive to the stress imposed by intense exercise, and the majority of cases of fibrosis detected in athletes are located in this ventricle, especially in the area that is in contact with the septum separating the two ventricles of the heart.
The presence of these fibrotic areas can in principle disturb the electrical signal and create a “short-circuit” that can cause rapid ventricular tachycardia, capable of degenerating into ventricular fibrillation (causing sudden death). It would therefore be possible that myocardial fibrosis, which preferentially affects endurance athletes, could play a role in the sudden death affecting some of them. In this sense, it should be noted that one study observed that marathon runners who presented an LGE signal were more at risk of cardiovascular events in the two years following diagnosis than athletes without an LGE signal, and another study observed ventricular arrhythmia in athletes with areas of fibrosis (at the level of the epicardium).
In sum, the studies carried out so far indicate that senior athletes who have done large volumes of high-intensity exercise for long periods of time are more likely to have fibrotic lesions in the myocardium. However, the consequences of these fibrosis remain uncertain given the low incidence of sudden cardiac death in this population, and because of studies showing that vigorous physical activity does not seem to increase the risk of ventricular arrhythmia and that people in excellent physical shape are at lower risk of premature mortality. For example, elite athletes (Olympic medallists, for example) live 3–6 years longer than the general population.
In conclusion, sudden cardiac death that occurs during a sports activity remains an extremely rare phenomenon, especially among senior athletes who are regularly active. The health benefits provided by physical activity thus far exceed the very slight risks involved in practising a sport. The amounts of exercise required to benefit the most from this protection are equivalent to approximately 1 hour of walking or ½ hour of running per day, which is far from excessive and represents a goal within reach of most people.
Very large volumes of intense exercise, such as those performed by high-level senior athletes, can induce certain cardiac abnormalities (coronary artery calcification, myocardial fibrosis), but the impact of these abnormalities on the risk of sudden death affecting these athletes remains uncertain. Large-scale prospective studies focusing specifically on athletes, for example the Master Athlete’s Heart study recently initiated in Europe, should make it possible to better identify the risk factors for sudden death in athletes.
In the current state of knowledge, the main risk factor for sudden death in athletes seems to be the same as that of the general population, i.e., the presence of an underlying coronary artery disease which blocks the supply of blood to the heart muscle. For example, in the study of sudden deaths during triathlons, researchers found that 30% of deceased athletes had signs of advanced coronary atherosclerosis. Putting on running shoes every morning does not completely prevent the development of coronary plaques and above all does not eliminate the atherosclerosis that has developed over the years. This is particularly true for athletes who have adopted sports later in life, after having had a suboptimal lifestyle (sedentary lifestyle, smoking, poor diet) for several years. Like the general population, senior athletes who regularly engage in large volumes of exercise and/or participate in endurance events therefore have every advantage in controlling well-established risk factors for atherosclerosis, such as cholesterol levels, blood pressure and type 2 diabetes.
We should also not neglect certain factors such as electrolyte imbalances (hyponatremia, in particular), heat stroke or pure and simple exhaustion which can alter cardiac function, regardless of the state of health of the coronaries. These factors cause intense physiological stress that could explain why the vast majority of deaths that occur during marathons occur in the last quarter of the race